
![]()
При посиланні на статтю з нашого журналу
необхідно вказувати:
- назву журналу
українською мовою - Медичні перспективи
або транслітерацією - Medicni perspektivi
- DOI статті
![]()


Медичні перспективи. 2026. Т. 31, № 1
2026 Том XXXI № 1
Опубліковано
31-03-2026
Ключові слова: громадське здоров’я, симуляційні технології, готовність до надзвичайних ситуацій, національна безпека, кризове реагування, симуляційне навчання
Key words: public health, simulation technologies, emergency preparedness, national security, crisis response, simulation-based training
Реферат
Система громадського здоров’я України функціонує в умовах поєднання воєнних загроз, інтенсивних міграційних процесів, трансформації соціального середовища та зростання ризиків біологічних, хімічних і техногенних інцидентів. За таких обставин традиційні освітні й управлінські підходи є обмеженими для формування готовності до комплексних кризових ситуацій і не дозволяють повною мірою оцінити спроможність системи до скоординованого реагування. У відповідь на ці виклики симуляційні технології дедалі частіше розглядаються як інструмент, що поєднує підготовку персоналу з тестуванням управлінських рішень і міжвідомчої взаємодії в безпечному середовищі. Метою роботи є концептуально-аналітичне узагальнення сучасних підходів до використання симуляційних технологій у сфері громадського здоров’я та формування прикладної рамки їх інтеграції для підвищення готовності й функціональної стійкості національної системи громадського здоров’я України до сучасних і комбінованих загроз. Аналіз ґрунтувався на опрацюванні рецензованих наукових публікацій, міжнародних методологічних рекомендацій і стратегічних документів, відібраних у міжнародних наукометричних базах даних та на офіційних ресурсах провідних міжнародних інституцій, переважно за період 2018-2025 років. Обґрунтовано доцільність розгляду симуляційних технологій не лише як освітнього інструмента, а як складової забезпечення системної готовності та функціональної стійкості громадського здоров’я. Систематизовано основні напрями застосування симуляцій, зокрема реагування на надзвичайні ситуації, тестування управлінських політик, кризову комунікацію та міжвідомчу координацію. Узагальнено роль медичних університетів як інституційної основи розвитку симуляційної підготовки та ідентифіковано ключові бар’єри її впровадження, включно з інфраструктурними, нормативними й методичними обмеженнями. На підставі отриманих аналітичних узагальнень сформульовано стратегічні напрями розвитку симуляційних технологій у системі громадського здоров’я України, реалізація яких розглядається як передумова підвищення готовності системи до сучасних і майбутніх загроз.
Abstract
Simulation as a tool for strengthening the preparedness of Ukraine’s public health system to threats: challenges and prospects. Miasoiedov V.V., Merkulova T.V., Nesterenko V.G., Peresypkina T.V. The public health system of Ukraine operates under a combination of military threats, intensive migration processes, transformation of the social environment, and increasing risks of biological, chemical, and technological incidents. Under these conditions, traditional educational and managerial approaches are limited in their capacity to ensure preparedness for complex crisis situations and do not allow for a comprehensive assessment of the system’s ability to respond in a coordinated manner. In response to these challenges, simulation technologies are increasingly considered as a tool that integrates workforce training with the testing of managerial decisions and intersectoral coordination in a safe environment. The aim of this study is a conceptual and analytical synthesis of contemporary approaches to the use of simulation technologies in public health and the development of an applied framework for their integration to enhance the preparedness and functional resilience of the national public health system of Ukraine to modern and combined threats. The analysis was based on peer-reviewed scientific publications, international methodological guidelines, and strategic documents retrieved from international scientific databases and official resources of leading international institutions, primarily covering the period from 2018 to 2025. The study substantiates the relevance of considering simulation technologies not only as an educational tool but as a component of ensuring systemic preparedness and functional resilience in public health. The main areas of application of simulations are systematized, including emergency response, testing of public policies, crisis communication, and intersectoral coordination. The role of medical universities as an institutional foundation for the development of simulation-based training is summarized, and key barriers to implementation are identified, including infrastructural, regulatory, and methodological constraints. Based on the analytical synthesis, strategic directions for the development of simulation technologies in the public health system of Ukraine are formulated, the implementation of which is considered a prerequisite for strengthening system preparedness for current and future threats.
Сучасні умови функціонування системи громадського здоров’я України формуються під впливом поєднання воєнних загроз, інтенсивних міграційних процесів, трансформації соціального середовища та зростання ризиків біологічних, хімічних і техногенних інцидентів [1]. За таких обставин традиційні підходи до підготовки фахівців й оцінювання інституційної готовності є обмеженими, оскільки не відтворюють багатофакторний і динамічний характер сучасних загроз. У відповідь на це в країнах з розвиненими системами безпеки дедалі ширше застосовуються симуляційні технології, які дозволяють моделювати кризові сценарії без ризику для населення та інфраструктури, поєднуючи підготовку персоналу з тестуванням управлінських механізмів [2, 3].
У сучасній практиці симуляція виходить за межі суто освітнього інструмента й розглядається як компонент забезпечення функціональної готовності систем громадського здоров’я та національної безпеки. Використання симуляцій дає змогу оцінювати реалістичність алгоритмів реагування, виявляти прогалини в міжвідомчій координації, перевіряти управлінські рішення та формувати поведінкові компетентності, необхідні для роботи в умовах невизначеності [4, 5, 6, 3]. Аналітичні огляди й дослідження у сфері громадського здоров’я та управління надзвичайними ситуаціями підтверджують доцільність розгляду симуляції як інструмента доказового управління, що дозволяє оцінювати ефективність організації реагування до настання реальних подій [7, 2, 3].
Важливим є також поведінковий і психоемоційний аспект симуляційного навчання. Дані міжнародних досліджень свідчать, що участь у симуляційних тренінгах підвищує впевненість фахівців, покращує командну взаємодію та знижує рівень тривожності в кризових ситуаціях, що безпосередньо впливає на якість управлінських рішень [8, 9]. Для України, де система громадського здоров’я одночасно реагує на наслідки воєнних дій, цивільні надзвичайні ситуації та загрози біобезпеці, ці характеристики набувають особливого значення.
У статті проаналізовано можливості та обмеження впровадження симуляційних технологій у систему громадського здоров’я України, обґрунтовано їх стратегічну роль, визначено потенціал університетів і міжнародного партнерства у формуванні національної моделі симуляційної підготовки, а також окреслено ризики, що потребують нормативного й наукового врегулювання.
Метою роботи є узагальнення сучасних підходів до використання симуляційних технологій у сфері громадського здоров’я як інструмента системної готовності та функціональної стійкості, а також формування прикладної концептуальної рамки інтеграції симуляцій у національну систему громадського здоров’я України в умовах сучасних і комбінованих загроз із визначенням ключових стратегічних напрямів їх подальшого розвитку.
МАТЕРІАЛИ ТА МЕТОДИ ДОСЛІДЖЕНЬ
Роботу виконано у форматі концептуально-аналітичного огляду проблеми з елементами картування доказів. Дизайн обрано з огляду на фрагментарність наявних наукових публікацій щодо використання симуляції саме в системі громадського здоров’я: більшість досліджень зосереджені або на клінічній симуляції, або на окремих компонентах готовності, тоді як комплексні емпіричні дослідження на стику «симуляція – громадське здоров’я – системна готовність» представлені обмежено. Методологічний підхід спрямований на узагальнення наявних наукових і нормативно-методичних джерел, їх тематичний аналіз та формування прикладної концептуальної рамки, релевантної для умов України.
Пошук літератури здійснено в міжнародних наукових базах даних PubMed, Scopus та Web of Science; додатково проведено цільовий пошук керівництв, практичних настанов і стратегічних документів на офіційних ресурсах міжнародних інституцій (зокрема ВООЗ і Європейського центру профілактики і контролю захворювань) та в національних нормативних і стратегічних документах України.
Для формування вибірки використовувались комбіновані пошукові запити українською та англійською мовами, анотації та ключові слова, які охоплювали теми громадського здоров’я, безпеки здоров’я, готовності та стійкості системи охорони здоров’я, симуляційних вправ, включно з післядієвим аналізом, а також компоненти підготовки кадрів, управлінських рішень, політик, координації та кризових комунікацій; окремо застосовано уточнювальні запити, пов’язані з підходом «Єдине здоров’я» (One Health). Часовим інтервалом відбору джерел були 2018-2025 рр., з можливістю включення окремих базових концептуальних джерел, опублікованих раніше. З вибірки виключено роботи, що описували виключно клінічну симуляцію без зв’язку із системною готовністю та управлінням у громадському здоров’ї, освітні або інформаційні матеріали без методичного обґрунтування й аналітичної цінності, дублікати, а також короткі повідомлення або новини без емпіричних чи аналітичних даних. Узагальнення виконували шляхом тематичного синтезу й рамкового аналізу з опорою на цикл готовності «підготовка – реагування – оцінка – покращення». Для кожного джерела структуровано вилучали інформацію про тип симуляційної вправи, мету застосування, рівень системи, наявність формалізованого оцінювання та потенціал адаптації до умов України.
Систематизацію джерел й описове картування (розподіл за типом джерела, тематичними напрямами та роком публікації) виконано із застосуванням електронних таблиць (Microsoft Excel/Google Sheets); статистичні гіпотези не тестувалися, оскільки дизайн роботи є концептуально-аналітичним оглядом.
Дослідження не передбачало залучення людей як об’єктів дослідження, використання персональних або чутливих медичних даних, у зв’язку з цим етичне схвалення не вимагалося.
РЕЗУЛЬТАТИ ТА ЇХ ОБГОВОРЕННЯ
Результати дослідження ґрунтуються на тематичному синтезі та рамковому аналізі відібраних джерел і відображають концептуальні підходи та закономірності застосування симуляцій у системі громадського здоров’я, а не кількісну оцінку ефектів чи показників.
У межах цієї роботи ключові поняття використовуються в такому значенні. Під готовністю системи громадського здоров’я розуміється спроможність інституцій, кадрового потенціалу та організаційних процесів завчасно планувати, здійснювати підготовку і тренування, реалізовувати реагування та забезпечувати відновлення функцій під час або після надзвичайних подій і загроз із застосуванням циклу безперервного покращення, зокрема через симуляційні вправи та післядієвий аналіз із подальшими планами удосконалення [2].
Функціональна стійкість системи громадського здоров’я в цій статті розглядається як здатність системи зберігати критично важливі функції – епідеміологічний нагляд, лабораторну діагностику, координацію, комунікацію та ухвалення управлінських рішень – в умовах підвищеного навантаження, а також оперативно відновлювати їх, використовуючи уроки, отримані під час симуляційних вправ або реальних подій.
Симуляція або симуляційна вправа в громадському здоров’ї визначається як структурована діяльність з моделювання сценаріїв загроз, що реалізується у форматі настільних, функціональних або повномасштабних вправ і призначена для підготовки та/або перевірки компонентів готовності системи з обов’язковим етапом оцінювання результатів і подальшого покращення.
Термін «симуляційна модель» у межах цього дослідження використовується як концептуальна рамка проєктування та вбудовування симуляційних вправ у цикл готовності системи громадського здоров’я.
Інтеграція симуляцій у громадське здоров’я: від освітньої функції до інструмента державної готовності
Інтеграція симуляцій у практику громадського здоров’я розширює можливості підготовки персоналу порівняно з традиційними освітніми форматами, оскільки забезпечує відпрацювання поведінкових й управлінських навичок, критично важливих для готовності системи до реагування [2, 8]. На відміну від лекційних і семінарських занять, симуляційні вправи відтворюють ситуації дефіциту часу та невизначеності, у яких фахівці мають приймати рішення, координувати командну взаємодію, застосовувати алгоритми кризових комунікацій і діяти в умовах динамічної зміни обстановки [3, 5, 6]. Це робить симуляцію ефективним інструментом підготовки кадрів громадського здоров’я та суміжних секторів, зокрема епідеміологів, фахівців первинної ланки, управлінців, лабораторних працівників, представників місцевого самоврядування та комунікаційних команд [10, 3].
Український контекст зумовлює потребу в сценаріях, що виходять за межі класичних інфекційних спалахів і враховують комбіновані загрози, у яких поєднуються хімічні, радіаційні, техногенні та біологічні компоненти. В умовах військової агресії, яка триває, симуляції дозволяють моделювати ситуації, у яких рішення ухвалюються за високого рівня невизначеності та стресу, а також перевіряти функціональну стійкість системи громадського здоров’я за одночасної дії кількох типів небезпек. До таких сценаріїв належать, зокрема, інфекційний спалах в умовах масової евакуації або руйнування критичної інфраструктури, а також комбіновані події, що потребують скоординованих дій різних служб і секторів [11, 12, 13]. У цьому сенсі симуляційні вправи виконують не лише освітню, а й інструментальну функцію, як механізм перевірки операційної готовності та міжвідомчої взаємодії в умовах кризових навантажень [14, 2].
Узагальнення ролі симуляцій у системі громадського здоров’я подано у вигляді концептуальної моделі (рис.), що поєднує лінійний та циклічний виміри. Лінійний компонент відображає логіку переходу від контексту загроз до результатів на рівні готовності та функціональної стійкості системи, тоді як циклічний – механізм безперервного покращення через симуляційні вправи, оцінювання та корекцію управлінських рішень.
Рисунок. Концептуальна модель ролі симуляцій у формуванні готовності та функціональної стійкості системи громадського здоров’я ↓
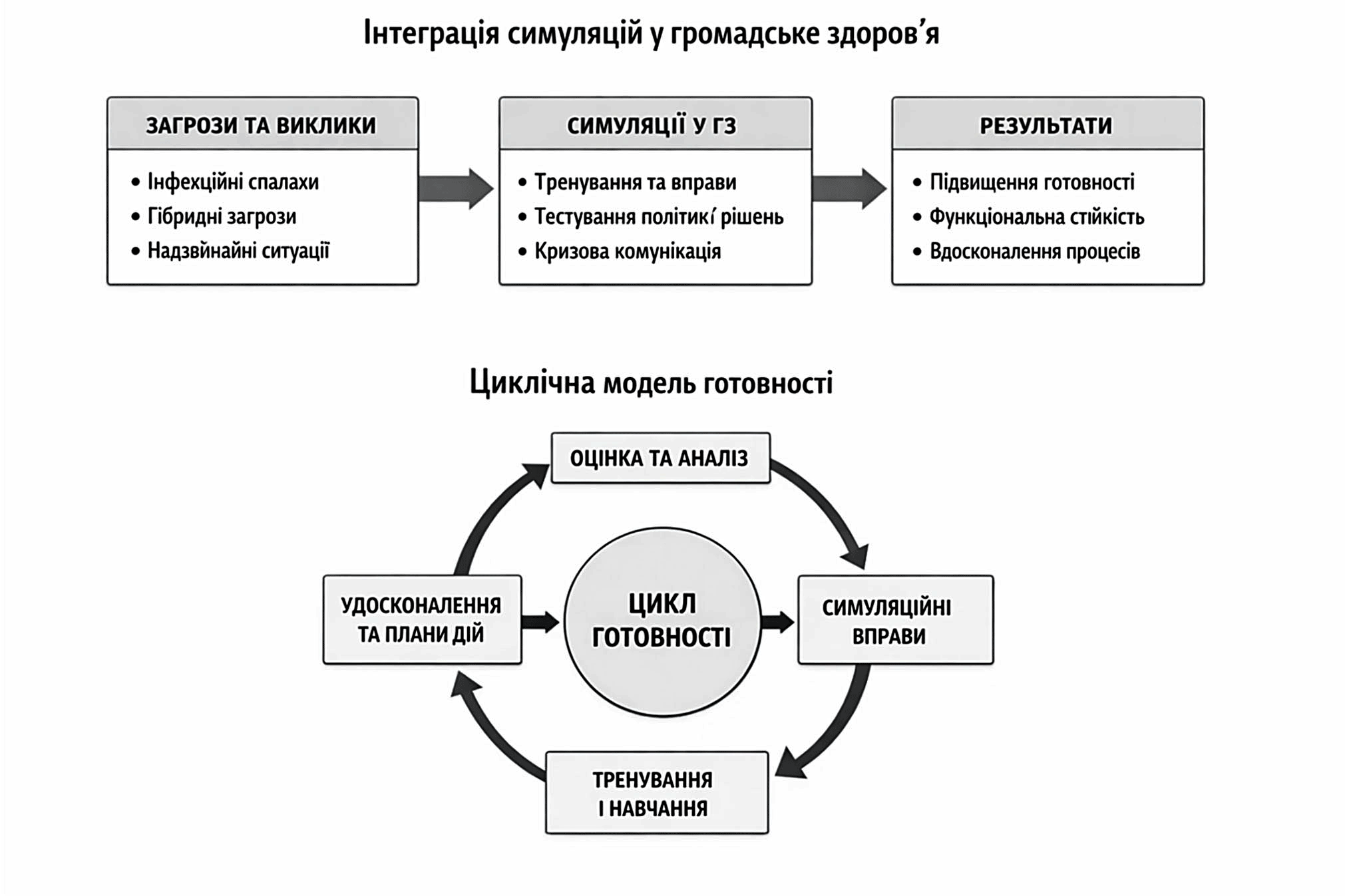
У міжнародній практиці симуляція також використовується як метод оцінювання операційної сумісності між службами. Методологічні документи Всесвітньої організації охорони здоров’я та Європейського центру профілактики і контролю захворювань передбачають застосування настільних, функціональних і повномасштабних вправ для перевірки ефективності системи реагування [3, 4, 5]. В Україні ці підходи поки застосовуються обмежено, переважно в контексті проєктних активностей або окремих навчань. Водночас регулярність симуляційних вправ є умовою підтримання узгодженості дій між структурами, які в повсякденній практиці взаємодіють нерегулярно, та підвищення готовності системи до скоординованого реагування [2, 3, 14].
Симуляція як інструмент формування поведінкових й управлінських компетентностей
Фахові дослідження та огляди останніх років у галузі симуляційної педагогіки, кризового менеджменту та підготовки фахівців громадського здоров’я свідчать, що симуляційні тренінги впливають насамперед на поведінкові та управлінські компетентності, критично важливі для ефективного кризового менеджменту, зокрема стратегічне мислення, лідерство, ухвалення рішень у стресових умовах, кризову комунікацію, орієнтацію на результат і толерантність до невизначеності [15, 16, 7, 8, 9]. Формування цих компетентностей відбувається переважно в середовищі, наближеному до реальних умов реагування, що обмежено або недосяжно в межах традиційних освітніх форматів.
Особливо значущою є роль симуляцій у підготовці епідеміологічних і лабораторних фахівців, діяльність яких пов’язана з раннім виявленням загроз, проведенням епідемічних розслідувань, визначенням випадку, управлінням даними та кризовими комунікаціями [10, 15]. Симуляційні вправи дозволяють відпрацювати повну траєкторію реагування – від фіксації первинних сигналів до ухвалення управлінських рішень щодо запровадження обмежувальних заходів або інформування населення – у логіці, наближеній до реального функціонування системи [3-5].
Вагомим компонентом впливу симуляцій є також формування психологічної готовності фахівців. Дані досліджень показують, що тренінги з елементами стрес-моделювання сприяють підвищенню впевненості, зменшенню тривожності та покращенню здатності працювати в багатопрофільних командах [8, 9]. В умовах тривалих кризових навантажень і війни цей аспект набуває стратегічного значення, оскільки безпосередньо впливає на здатність системи громадського здоров’я зберігати працездатність і підтримувати узгоджені дії персоналу.
Медичні університети як ядро розвитку симуляційних технологій
Система медичної освіти України розглядається як одна з ключових інституційних основ для розвитку національної моделі симуляційної підготовки у сфері громадського здоров’я. На відміну від відомчих структур, медичні університети поєднують освітню, наукову та методичну функції, що створює умови для системного впровадження симуляційних технологій. Університети можуть забезпечувати підготовку тренерів за моделлю підготовки інструкторів (train-the-trainer), розроблення та апробацію симуляційних сценаріїв, науковий супровід безпечності й ефективності симуляційного середовища, а також формування кадрового резерву для системи безперервного професійного розвитку фахівців [17, 18, 5].
Заклади вищої освіти мають можливість інтегрувати симуляційні технології в освітні компоненти програм медичних і медико-соціальних спеціальностей, забезпечуючи формування компетентностей – від базових клінічних і комунікаційних до навичок міжвідомчої взаємодії у складних кризових сценаріях [8, 16, 18]. Такий підхід узгоджується з європейськими моделями підготовки, у яких симуляція розглядається як невід’ємний елемент освіти та підвищення кваліфікації фахівців, залучених до охорони здоров’я та управління ризиками [19, 3].
Міжнародний досвід: можливості адаптації для України
У міжнародній практиці симуляційні методи розглядаються як інструмент підвищення готовності та запобігання кризам, а не лише як елемент навчання. У низці країн симуляційні центри та програми використовуються для тестування управлінських рішень, міжпрофесійної взаємодії та операційної сумісності служб у кризових сценаріях [2, 3]. У Європейському Союзі симуляційні вправи інтегровані в механізми оцінювання готовності систем громадського здоров’я, а міждержавні симуляційні вправи (Simulation Exercises, SimEx), що регулярно проводяться Європейським центром з профілактики та контролю захворювань, слугують інструментом перевірки координації та узгодженості реагування [20, 21]. На глобальному рівні підходи ВООЗ передбачають використання результатів симуляцій і післядієвого аналізу для корекції політик і планів реагування на основі принципу ідентифікованих уроків (lessons identified) [4]. У сукупності ці практики формують рамку, що може бути адаптована в Україні, зокрема в частині створення міжвідомчих платформ для спільного навчання, аналізу рішень і підвищення операційної готовності.
Окремий аналітичний інтерес для України становить модель One Health, яка ґрунтується на міжсекторальній взаємодії систем охорони здоров’я, ветеринарної медицини та охорони довкілля і підтримується провідними міжнародними організаціями. Практика проведення One Health Simulation Exercises демонструє ефективність спільного відпрацювання сценаріїв для служб громадського здоров’я, безпеки харчових продуктів і ветеринарії, особливо в умовах зоонозних і комбінованих загроз [22, 11, 12, 13]. Наявний в Україні базовий досвід міжсекторальних тренінгів за підтримки ВООЗ і партнерських структур створює передумови для подальшого інституційного закріплення та масштабування таких підходів на національному рівні [4, 5].
Бар’єри впровадження та ризики, що потребують системної відповіді
Інтеграція симуляційних технологій у систему громадського здоров’я України стримується не окремими ізольованими проблемами, а сукупністю структурних і нормативних обмежень, які формують системний бар’єр для їх масштабування та сталого використання. Ці обмеження стосуються інфраструктурного забезпечення, регуляторного середовища та механізмів оцінювання результатів симуляційної підготовки.
Однією з ключових проблем є нерівномірний розвиток симуляційної інфраструктури та обмежений доступ до відповідних ресурсів у регіонах, що ускладнює формування єдиного підходу до підготовки кадрів і міжвідомчої взаємодії. Фрагментарність цифрових рішень і відсутність інтегрованих платформ додатково знижують можливості координації, накопичення результатів та аналітичного використання даних симуляційних вправ [23, 14].
Вагомим регуляторним викликом залишається відсутність нормативно визначених вимог до безпечності та якості симуляційного середовища. Зокрема, в Україні не сформовано чітких стандартів щодо гігієнічних, психофізіологічних і когнітивних навантажень, пов’язаних з моделюванням критичних ситуацій. Із розширенням використання технологій віртуальної та доповненої реальності ці прогалини набувають додаткового значення, оскільки зростають ризики емоційної небезпеки, когнітивного перевантаження та ергономічних порушень, які наразі недостатньо досліджені й регламентовані [24, 25, 26].
Окремим системним обмеженням є відсутність уніфікованого підходу до оцінювання результатів симуляційних тренінгів і державного обліку їх проходження. Це унеможливлює повноцінну інтеграцію симуляцій у національну систему безперервного професійного розвитку, а також обмежує використання результатів симуляцій для планування кадрової політики, оцінювання готовності та обґрунтування управлінських рішень у сфері громадського здоров’я [4, 5].
Цифрова інфраструктура симуляційної підготовки
Формування національної моделі симуляцій у громадському здоров’ї потребує розвитку цифрової інфраструктури, яка забезпечує не лише проведення симуляційних вправ, а й їх координацію, документування та аналітичне використання результатів. У цьому контексті цифрові рішення розглядаються як інструмент масштабування симуляцій і підтримки системної готовності, а не як окремий технологічний компонент.
Ключовим елементом такої інфраструктури може бути віртуальна симуляційна платформа з національним репозиторієм сценаріїв, що дозволяє організовувати віддалені та змішані формати симуляцій, уніфікувати сценарії, накопичувати результати вправ і забезпечувати порівнюваність підходів до підготовки фахівців [4, 25, 26]. Наявність спільного цифрового середовища створює умови для узгодженого використання симуляційних сценаріїв і результатів між освітніми, науковими та практичними інституціями, залученими до функціонування системи громадського здоров’я [3, 18].
Окрім освітньої складової, цифрова інфраструктура розширює можливості використання симуляцій як інструмента аналізу та тестування управлінських рішень. Моделювання сценаріїв у цифровому середовищі дозволяє оцінювати потенційні наслідки управлінських алгоритмів і політичних рішень до їх реалізації в реальних умовах, що відповідає міжнародним практикам доказового ухвалення рішень у сфері громадського здоров’я та кризового управління [2, 19].
Стратегічні напрями розвитку симуляційних технологій у громадському здоров’ї
Подальший розвиток симуляційних технологій у сфері громадського здоров’я доцільно розглядати як перехід від фрагментарних освітніх ініціатив до цілісної, стандартизованої та науково обґрунтованої національної моделі, інтегрованої в систему підготовки кадрів, оцінювання готовності та формування політик. Узагальнення виявлених бар’єрів і міжнародних підходів дозволяє окреслити ключові стратегічні напрями такого розвитку.
Першим стратегічним напрямом є формування модульної системи симуляційної підготовки для різних категорій фахівців громадського здоров’я та суміжних секторів. Модульність дозволяє поєднувати базові та поглиблені сценарії реагування на інфекційні, техногенні, хімічні, радіаційні й комбіновані загрози з урахуванням професійних ролей і рівнів відповідальності.
Другим напрямом є інтеграція симуляцій у систему безперервного професійного розвитку як інструмента не лише навчання, а й перевірки та підтримання професійної готовності. Використання результатів симуляційних вправ у межах офіційних програм підвищення кваліфікації створює передумови для формування прогнозованої моделі розвитку кадрового потенціалу.
Третім стратегічним напрямом є розвиток національної мережі тренерів за моделлю «train-the-trainer». Підготовка сертифікованих інструкторів, здатних забезпечувати проведення симуляцій, адаптацію сценаріїв і методичний супровід у регіонах, є необхідною умовою масштабування симуляційних технологій і забезпечення рівного доступу до них.
Четвертий напрям стосується формування методичної та нормативної бази симуляційної підготовки. Йдеться про розроблення уніфікованих вимог до структури симуляційних вправ, критеріїв оцінювання результатів і стандартів безпечності симуляційного середовища, що забезпечують порівнюваність підходів і підвищення якості підготовки.
П’ятим напрямом є науковий супровід розвитку симуляційних технологій. Систематичні дослідження ефективності різних форматів симуляцій, валідності інструментів оцінювання та впливу симуляційного середовища на психофізіологічний стан учасників формують доказову основу для вдосконалення практик і стандартів.
Шостий стратегічний напрям пов’язаний з розвитком цифрових інструментів симуляційної підготовки, включно з віддаленими, змішаними та віртуальними форматами. Цифрові рішення розглядаються як інфраструктурна основа для масштабування симуляцій, уніфікації сценаріїв й аналітичного використання результатів.
Сьомим напрямом є посилення міжвідомчої координації шляхом впровадження симуляційних вправ за участю не лише системи охорони здоров’я, а й служб надзвичайних ситуацій, лабораторних, освітніх і соціальних інституцій. Такий підхід сприяє формуванню узгоджених алгоритмів реагування та підвищує здатність системи громадського здоров’я діяти в умовах комплексних криз.
Запропоновані стратегічні напрями узгоджуються із сучасними міжнародними підходами до використання симуляцій як інструмента підвищення готовності та функціональної стійкості систем громадського здоров’я й можуть слугувати основою для подальшого розвитку національної моделі симуляційної підготовки.
Обмеження дослідження: дослідження має обмеження, пов’язані з його концептуально-аналітичним характером, оскільки висновки ґрунтуються на узагальненні наукових і методичних джерел та не передбачають емпіричної перевірки або кількісної оцінки ефективності симуляційних інтервенцій.
ВИСНОВКИ
Проведений аналіз дозволив сформулювати такі узагальнення:
Внески авторів:
М’ясоєдов В.В. – концептуалізація, адміністрування проєкту;
Меркулова Т.В. – методологія, дослідження, написання – початковий проєкт;
Нестеренко В.Г. – формальний аналіз, курація даних;
Пересипкіна Т.В. – написання – рецензування та редагування, візуалізація.
Фінансування. Дослідження не має зовнішніх джерел фінансування.
Конфлікт інтересів. Автори заявляють про відсутність конфлікту інтересів.
REFERENCES
Key words: hard capsules, quality control, Ishikawa diagram, critical parameters, technology
Ключові слова: тверді капсули, контроль якості, діаграма Ішікави, критичні параметри, технологія
Abstract
This article explores the application of the Ishikawa (cause-and-effect) diagram as a risk analysis tool within a pharmaceutical quality system for the production of hard capsules under the code name "Praziquantel Plus". Aligned with the standards of ISO 9001, ICH Q10, and GMP, the study demonstrates how this method systematically identifies and analyzes potential risks across key production categories. The research provides a tailored Ishikawa diagram that facilitates the identification of critical parameters, supports process optimization, and enhances the overall quality assurance system for this specific medicinal product. The aim of the research was to analyze the risks in the production of hard capsules under the conditional name “Praziquantel Plus” using the Ishikawa diagram. The study was based on the analysis of a model industrial process for the production of Praziquantel Plus hard capsules. The materials for the risk analysis were the technological regulations, specifications for raw materials and finished product, as well as the requirements of GMP/ICH standards. The study employed a systematic approach to risk assessment in accordance with ICH Q9 guidelines. The primary methodology is centered on the construction of the Ishikawa diagram. The study is based on a systems approach, brainstorming, cluster analysis and cause-and-effect analysis. A comprehensive Ishikawa diagram was developed, structured around six primary risk categories for pharmaceutical production: raw materials, production process, equipment, personnel, premises, and quality control. Critical risk factors were identified and prioritized. The most significant risks were found to be associated with: a) the quality of active pharmaceutical ingredients and excipients (e.g., inconsistency in quantitative content, impurities); b) critical stages of the technological process (e.g., weighing accuracy, mixture homogeneity, capsule filling flowability); and c) the specifics of pharmaceutical equipment qualification and operation. Detailed risk assessment tables were created for both raw materials and the technological process, outlining potential failures, their consequences, and proposed precautionary measures to mitigate each risk (e.g., enhanced incoming quality control, process validation, equipment calibration). An adapted, product-specific Ishikawa diagram was proposed for the industrial-scale production of “Praziquantel Plus”. This diagram details first- and second-order subcategories within the main "bones," reflecting the unique aspects of scaling up from laboratory to commercial manufacturing. The Ishikawa diagram method proves to be an effective and structured tool for pre-emptive risk identification in pharmaceutical process development and scale-up, aligning with GMP and ICH Q9/Q10 requirements. The study successfully mapped and systematized the key risk categories and their interrelations for the production of “Praziquantel Plus” hard capsules, providing a visual and analytical framework for quality management. The proposed tailored diagram and risk tables serve as a practical foundation for implementing preventive actions, optimizing the technological process, and conducting root-cause analysis of potential defects, thereby strengthening the overall Pharmaceutical Quality System for this product.
Реферат
Аналіз ризиків у виробництві твердих капсул під умовною назвою «Празиквантел плюс» методом діаграми Ішікави. Семченко К.В., Яковенко В.К., Шмалько О.О., Олійник С.В. У цій статті досліджується застосування діаграми Ішікави як інструменту аналізу ризиків у фармацевтичній системі якості для виробництва твердих капсул під умовною назвою «Празиквантел Плюс». Відповідно до стандартів ISO 9001, ICH Q10 та GMP, показано, як цей метод систематично виявляє та аналізує потенційні ризики в ключових категоріях виробництва. Запропоновано адаптовану діаграму Ішікави, яка полегшує ідентифікацію критичних параметрів, підтримує оптимізацію процесів та покращує загальну систему забезпечення якості для цього конкретного лікарського засобу. Мета цього дослідження полягала в аналізі ризиків у виробництві твердих капсул під умовною назвою «Празиквантел Плюс» за допомогою діаграми Ішікави. Дослідження ґрунтувалося на аналізі модельного промислового процесу виробництва твердих капсул «Празиквантел Плюс». Матеріалами для ризик-аналізу слугували технологічний регламент, специфікації на сировину та готовий продукт, а також вимоги стандартів GMP/ICH. У дослідженні було використано систематичний підхід до оцінювання ризиків відповідно до рекомендацій ICH Q9. Основна методологія зосереджена на побудові діаграми Ішікави. Дослідження базується на системному підході, мозковому штурмі, кластерному аналізі та причинно-наслідковому аналізі. Розроблено комплексну діаграму Ішікави, структуровану навколо шести основних категорій ризику для фармацевтичного виробництва: сировина, виробничий процес, обладнання, персонал, приміщення та контроль якості. Ідентифіковано та пріоритизовано критичні фактори ризику. Найбільш значущими виявилися ризики, пов'язані з: а) якістю АФІ та допоміжних речовин (напр., невідповідність кількісного вмісту, домішки); б) критичними етапами технологічного процесу (напр., точність зважування, однорідність суміші, сипкість маси при заповненні капсул); в) специфікою кваліфікації та експлуатації фармацевтичного обладнання. Створено детальні таблиці оцінки ризиків як для сировини, так і для технологічного процесу, де описані потенційні відмови, їх наслідки та запропоновані превентивні заходи для зменшення кожного ризику (напр., посилений вхідний контроль якості, валідація процесу, калібрування обладнання). Запропоновано адаптовану, продукт-специфічну діаграму Ішікави для промислового виробництва «Празиквантел Плюс». Ця діаграма деталізує підкатегорії першого та другого рівня в межах основних «кісток», що відображає особливості масштабування технології з лабораторного рівня на виробничий. Метод діаграми Ішікави зарекомендував себе як ефективний та структурований інструмент для превентивної ідентифікації ризиків при фармацевтичній розробці та масштабуванні процесів, що відповідає вимогам GMP та ICH Q9/Q10. Дослідження успішно систематизувало ключові категорії ризиків та їх взаємозв'язки для виробництва твердих капсул «Празиквантел Плюс», надавши візуальну та аналітичну основу для управління якістю. Запропоновані спеціалізована діаграма та таблиці ризиків слугують практичною основою для впровадження профілактичних дій, оптимізації технологічного процесу та аналізу основних причин потенційних дефектів, тим самим посилюючи загальну Фармацевтичну систему якості для цього препарату.
A Pharmaceutical Quality System (PQS) is a set of processes and procedures aimed at ensuring that pharmaceutical products are produced, stored and distributed in accordance with established quality standards. The basis of PQS is the international quality management system ISO 9001 and the requirements set out in the ICH Q10 guidelines. The system provides:
Quality of pharmaceutical products in Ukraine are regulated mainly by the requirements of State Pharmacopoeia of Ukraine, guidelines and the numerous orders of the Ministry of Health of Ukraine (MOHU) [1, 2, 3].
Risk analysis is a key component of PQS, which helps to minimize potential threats to product quality and patients. It is based on the principles outlined in the ICH Q9 guideline (“Quality Risk Management”). The main steps of risk analysis are risk identification, risk assessment, risk mitigation, risk monitoring and risk control.
Various methods are used to manage risks:
The Ishikawa diagram is an effective analytical tool for ensuring the quality of medicinal products. The main purpose of this method is to systematically identify and classify probable problems or causes of their occurrence in the production process. The use of the method is due to the complexity of the production of pharmaceutical products, when a combination of factors, such as the quality of incoming raw materials, equipment, technological methods, personnel, premises, etc., that can affect the quality of products both directly and indirectly.
The Ishikawa diagram gives the opportunity to structure the analysis process by highlighting the main categories of factors that can affect the quality of the medicinal product. This provides a comprehensive approach to solving problems, eliminating chaos in the search for causes. By detailing each category of factors, the root causes that lead to product defects, for example, uneven dosing of APIs in dosed preparations, can be identified. Usage of the diagram allows us to predict possible risks and create preventive measures aimed at improving production processes. This method admits enterprises to comply with high quality standards, such as the international Good Manufacturing Practice (GMP) standards and the international quality management system (ISO), ensuring quality control at all stages of production.
In scientific activities, the Ishikawa diagram construction method gives the opportunity to assess possible risks when scaling a laboratory technological process to a production one, establish possible critical parameters of the production process, and identify risks when developing quality control methods for medicinal products [4-8].
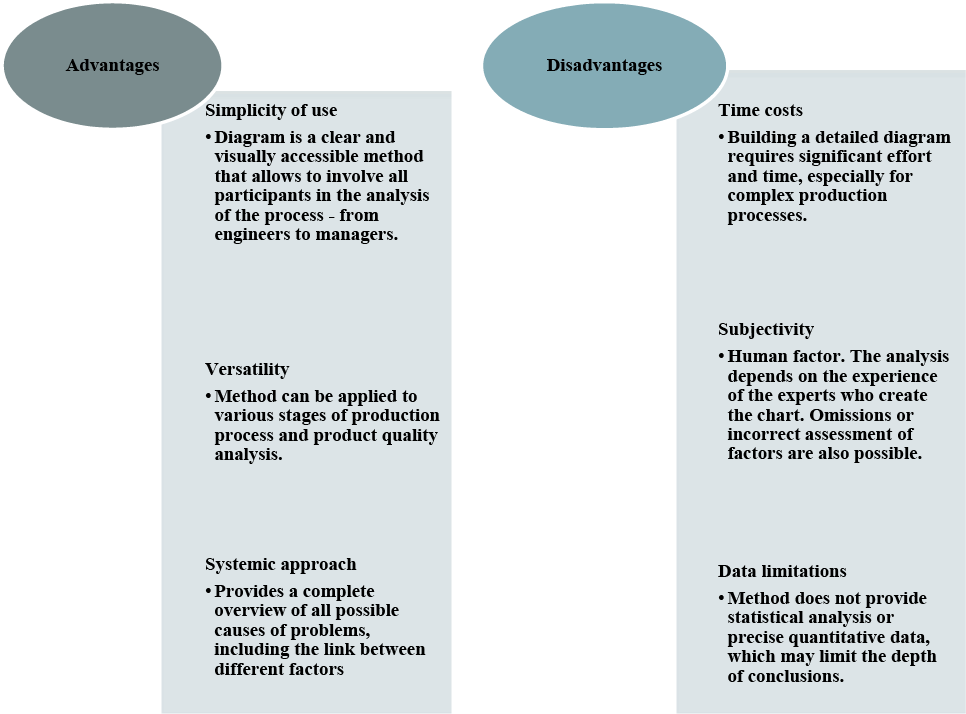
The Ishikawa diagram is an indispensable tool in pharmaceutical production, its usage contributes to the improvement of production processes, raising quality standards and preventing risks [9, 10]. However, it is important to consider the disadvantages of this method when combining it with other analytical tools for a deeper and more accurate analysis. The advantages and disadvantages of the Ishikawa diagram method are shown in Figure 1.
Fig. 1. Advantages and disadvantages of the Ishikawa diagram method ↓
The purpose of this study was to analyze the risks in the production of hard capsules under the conditional name “Praziquantel Plus” using the Ishikawa diagram.
MATERIALS AND METHODS OF RESEARCH
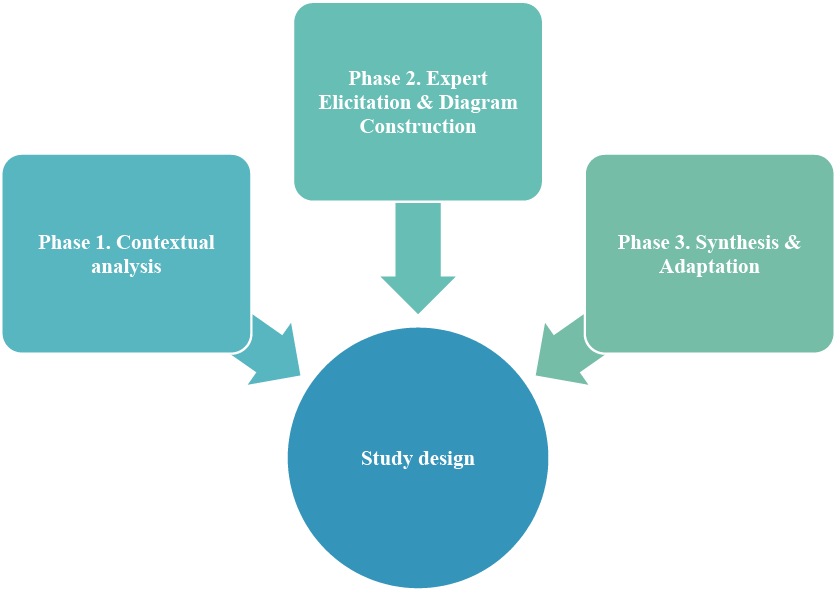
This research follows a qualitative, descriptive study design structured into three consecutive phases to ensure a systematic approach to risk identification and analysis (Fig. 2).
Phase 1: Contextual Analysis. A comprehensive review of the technological documentation for “Praziquantel Plus” capsules and relevant quality standards (GMP, ICH Q9, Q10) was conducted to define the scope and framework for risk assessment.
Phase 2: Expert Elicitation & Diagram Construction. The core analytical phase involved a structured brainstorming session with an expert panel (n=5) comprising pharmaceutical technologists, quality assurance, and production specialists. The elicited potential failure causes were then organized using cause-and-effect analysis and cluster analysis to construct a general Ishikawa diagram.
Phase 3: Synthesis & Adaptation. Based on the general diagram and a detailed process breakdown, a product-specific Ishikawa diagram for industrial-scale production was developed. Identified risks were further detailed and mitigation measures were proposed in tabular form.
Primary Analytical Tool. The Ishikawa (fishbone) diagram served as the primary visual and analytical tool throughout Phases 2 and 3 to structure and present the cause-and-effect relationships.
Fig. 2. Study design ↓
The basis for the study was the theoretical and information array necessary for modeling the risk analysis process. The materials of the study were a model technological process for the industrial production of hard capsules with combined content (code name “Praziquantel Plus”); a list of potential critical control points and quality parameters, identified based on the requirements of the State Pharmacopoeia of Ukraine, GMP and similar technologies; and categories of risk factors generally recognized in the pharmaceutical industry.
The study employed a systematic approach to risk assessment in accordance with ICH Q9 guidelines [2]. The primary qualitative methodology centered on the construction of an Ishikawa diagram. The process involved the following steps:
For risk prioritization, experts assessed each identified cause based on its estimated probability of occurrence and severity of impact on critical quality attributes. This qualitative assessment allowed for the identification of the most critical parameters requiring control measures, as presented in Tables 1 and 2.
For risk prioritization, a semi-quantitative approach based on the Risk Priority Number (RPN) was employed, in accordance with the principles of ICH Q9. Following the brainstorming session and construction of the general Ishikawa diagram, the expert panel (n=5) assessed each identified potential cause of failure.
Each risk was evaluated using two parameters:
Probability (P): The likelihood of the risk occurring.
Severity (S): The seriousness of the potential impact on the critical quality attributes (CQAs) of “Praziquantel Plus” capsules and patient safety.
Both parameters were scored on a 3-point ordinal scale (1=Low, 2=Medium, 3=High). The consensus scores were then multiplied to calculate the Risk Priority Number (RPN=P×S), which could range from 1 to 9.
Based on the RPN value, risks were prioritized for further analysis and mitigation:
High-priority (RPN≥6): Risks requiring immediate preventive actions and detailed control strategies (e.g., in-process controls, validation).
Medium-priority (RPN 3-4): Risks requiring monitoring and standard quality control procedures.
Low-priority (RPN 1-2): Acceptable risks under current control measures.
This prioritization enabled the research team to focus the subsequent detailed analysis on the “Raw Materials” and “Technological Process” categories, which contained over 70% of all high-priority risks.
Given the qualitative nature of the study and the use of expert elicitation data, formal statistical software was not employed for hypothesis testing. The semi-quantitative RPN calculation was performed using Microsoft Excel 365. Data organization and diagram structuring were supported by standard features of the software.
This study involved a structured expert elicitation session (brainstorming) as part of the risk analysis methodology. Participation was voluntary, and all experts provided informed verbal consent after being briefed on the study’s purpose and the anonymous, aggregated use of their input for academic publication. No personal or sensitive data were collected. The research procedure, focusing on process analysis rather than human subjects, was conducted in accordance with the ethical principles for non-interventional studies. Formal review by an institutional ethics committee was not required for this type of methodological research, as confirmed by the internal regulations of the National University of Pharmacy.
RESULTS AND DISCUSSION
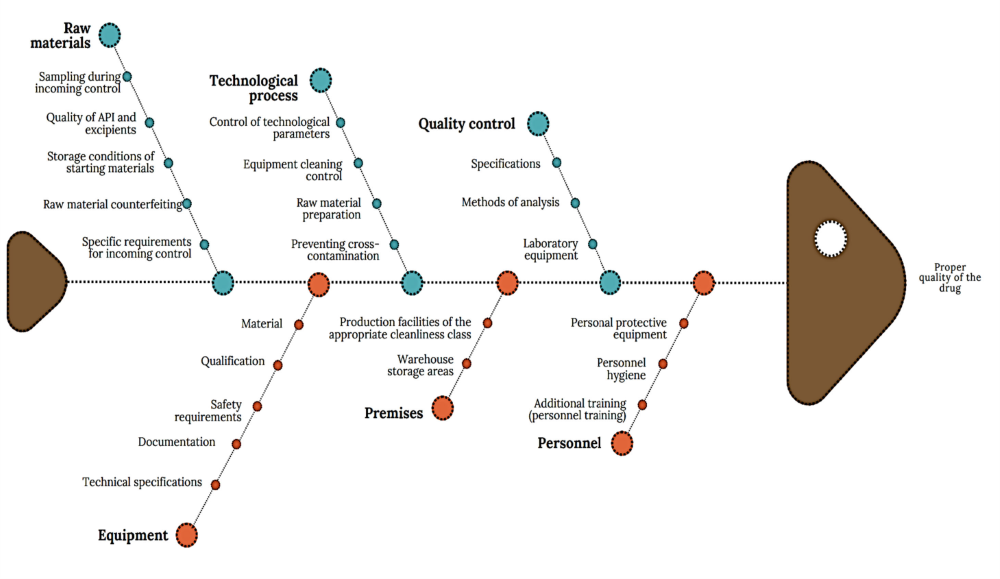
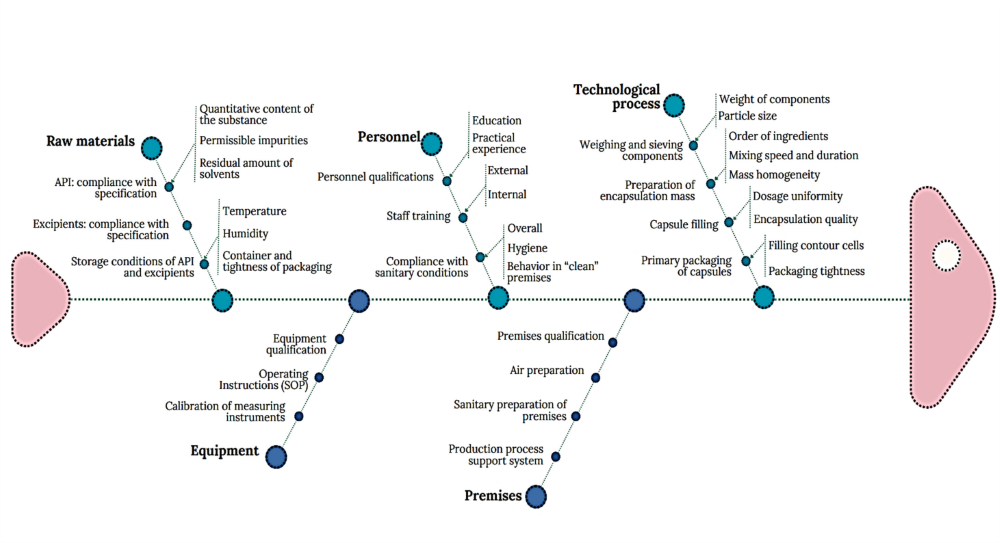
The general Ishikawa diagram, which allows taking into account the multilevel nature of factors affecting the quality of a drug as a final product and establishing key links between them, is shown in Figure 3. This diagram is based on the requirements of current legislation, WHO recommendations and national standards [11, 12].
According to the diagram (Fig. 3), the main risk factors of drug production include the quality of raw materials, technological process, quality control, premises, equipment, personnel, which are detailed by level 2 factors. Among the listed main factors, it is possible to distinguish factors of the first and second order in terms of significance, establish their links and group them.
1. Risk Prioritization and Justification of Focus
To move from a mere listing of factors to a justified conclusion about their criticality, a semi-quantitative risk assessment was performed. An expert panel (n=5) scored each identified cause from the general diagram (Fig. 3) on scales of Probability (P) and Severity (S) as described in the Methods. The calculated Risk Priority Number (RPN) served as a quantitative filter. The distribution of high-priority risks (RPN ≥6) across categories is presented in Fig. 3. As evidenced, the “Raw Materials” and “Technological Process” categories contained over 70% of all high-priority risks. This objective data directly supports our decision to focus the subsequent detailed analysis precisely on these areas, as presented in Tables 1 and 2 and in the adapted diagram (Fig. 4).
2. Detailed Analysis of High-Priority Risks
Following the prioritization, the most critical risks were analyzed in depth considering the peculiarities of production processes and the influence of factors on the quality of the finished drug, they can be divided into specific and general. Specific factors include the quality of the raw materials, quality control of the raw materials, intermediate and finished products, and the technological process. It is these factors that were subjected to the most thorough analysis during our study.
Of course, the main influence on the quality of the future drug is the quality of the raw material. Its quality risks are characterized by several secondary factors, illustrated in the diagram.
During the quality control of the finished drug, the choice of the API/excipient and the development of a method for its qualitative and quantitative determination, as well as the assessment of the microbiological state, are of great importance. All specification parameters are developed in accordance with the general guidance on finished drugs.
When conducting stability tests for drugs with several APIs, the possible mutual influence on the process of qualitative and quantitative determination of substances should be considered. Validation of the methods used is an urgent and mandatory task in the development of the MCQ.
Fig. 3. Diagram of cause-and-effect factors for ensuring the quality of medicines ↓
Factors such as premises and personnel have an unconditional impact on ensuring the quality of medicinal products. However, given the standardized requirements for both personnel and premises set out in the licensing conditions, we decided to specify only specific requirements for these factors. The main research was devoted to the input raw materials, technological process, quality control and equipment, which are decisive in the process of pharmaceutical development and introduction of new original medicinal products.
Production premises should follow a logical sequence of the production process. For both APIs and excipients, temperature and humidity control, filtration and effective ventilation are of great importance. Weighing of raw materials should be carried out in a separated from the production process premise. The design of the premises should facilitate compliance with special measures to prevent cross-contamination and facilitate cleaning when dust is generated (sampling, weighing, grinding, mixing, sieving and other operations). Warehouses should have sufficient capacity for orderly storage of different categories of raw materials. Containers should be placed in such a way as to ensure free air circulation. The storage area should provide protection of materials from weather conditions and control of proper storage conditions. Warehouses should have separate areas: for quarantined materials, approved materials and rejected starting materials.
Production personnel and quality control personnel must have special training. The authorized person must have specific knowledge of the processing and quality control of materials in the production of film-coated tablets. Strict adherence to hygiene requirements by personnel during the production process prevents further contamination of raw materials, intermediate products and finished products. Production personnel who are in direct contact with raw materials must be provided with personal protective equipment: masks, gloves, glasses. Persons with allergic diseases or predisposition to them are not allowed to work with raw materials.
Pharmaceutical equipment used must meet the requirements of good manufacturing practice. The operational characteristics of the equipment must ensure the performance of the production task within the operating load range. The technical characteristics of the equipment must correspond to the planned range and volumes of product output. The material of the equipment must not interact with the raw materials or products, serve as a source of contamination of the intermediate and finished product.
Qualification of critical equipment, process validation and change control ensure the reproducibility of the production process, thereby guaranteeing consistent quality and efficacy of different batches of the drug produced.
In order to minimize the potential risks of industrial production of hard capsules under the conditional name “Praziquantel Plus” when extrapolating laboratory technology, their analysis was conducted.
The main categories defined are raw materials, production process, equipment, personnel and premises. Particular attention was paid to potential risks associated with APIs and excipients (Table 1) and with the technological process (Table 2).
Taking into account the peculiarities of adapting laboratory technology to industrial conditions for the production of hard capsules under the conditional name “Praziquantel Plus”, the Ishikawa diagram focused on the peculiarities of the production process of this particular drug was constructed (Fig. 4). The categories “Raw materials”, “Technological process” and “Personnel” contain subcategories of the first and second order, maximally corresponding to the peculiarities of the production process of this drug.
The proposed Ishikawa diagram for hard capsules under the conditional name “Praziquantel Plus” can be used in the future in the following situations:
1. Analysis of the causes of product defects. If there is a problem with the quality of the capsules being produced (for example, capsules with uneven dosage), the diagram will help identify possible sources of the problem.
2. Quality control. The diagram will help to adjust the various stages of the production process to avoid defects at all stages of production.
3. Process optimization. Analyzing all possible causes of failures or costs during production allows to increase efficiency and reduce costs.
Fig. 4. Cause-and-effect diagram of quality assurance factors for hard capsules under the conditional name “Praziquantel Plus” ↓
The general cause-and-effect diagram constructed for our study identified six primary categories: Raw Materials, Technological Process, Quality Control, Premises, Equipment, and Personnel. This categorization is a direct operationalization of the integrated approach required by a PQS, as described in the ICH Q10 guideline. Furthermore, our systematic approach to risk identification, assessment, and control is fundamentally based on the principles of ICH Q9 (Quality Risk Management). While ICH Q9 provides the high-level framework, our study demonstrates its practical implementation by selecting an appropriate tool (Ishikawa diagram) for a specific, defined scope – the scale-up of a capsule product.
Our identification of raw material quality as a first-order risk factor (Table 1) is a universally acknowledged principle in Good Manufacturing Practice (GMP). The WHO in its GMP guidelines explicitly states that the quality of a finished product depends heavily on the quality of the starting materials.
Our detailed breakdown of the technological process resonates strongly with the findings of other researchers who have applied risk management to solid dosage forms. For instance, a review by Yu et al. (2014) [13] on the application of Quality by Design (QbD) to solid oral dosage forms identifies “blend uniformity” and “powder flow properties” as critical process parameters for capsule filling and tablet compression, which are directly related to our identified risks of “Heterogeneity of the encapsulation mass” and “Poor flowability of the mixture”. While Yu et al. approached this from a QbD perspective, our use of the Ishikawa diagram arrived at the same critical parameters, demonstrating the tool’s effectiveness in pinpointing areas that require rigorous control.
Similarly, the risk we identified concerning the “Weighing and Sieving” stage, particularly, inaccuracy in weighing, is highlighted in GMP literature as a common source of error. The PIC/S GMP Guide dedicates an entire annex to the Guidance on Good Manufacturing Practice for Medicinal Products, where it emphasizes that weighing, measuring, and other equipment used for critical steps should be calibrated and checked at defined intervals (5, Annex 4) [14].
Our analysis of the “Personnel” and “Premises” categories, while noting their standardized requirements, specified risks such as the need for personnel with special training and the exclusion of individuals with allergic predispositions. This aligns with the human factor engineering concepts increasingly integrated into GMP. The FDA's guidance on quality systems approaches emphasizes that as management should ensure that personnel have the education, training, and experience, or any combination thereof, to perform their assigned functions [15]. Our inclusion of a specific health screening (allergies) adds a nuanced, product-specific layer to this general personnel requirement, a detail that is often crucial in practice but may be absent from high-level guidelines.
Regarding “Premises”, our emphasis on a logical flow, separate weighing areas, and controlled warehouses to prevent contamination and mix-ups is a cornerstone of GMP facility design, as outlined by ISPE in its Baseline Guide: Oral Solid Dosage Forms [16]. Our use of the Ishikawa diagram effectively integrates these infrastructural and design requirements into the same risk assessment framework as the process parameters, promoting a holistic view of quality that is essential for successful pharmaceutical production.
Today, the pharmaceutical industry, following the automotive industry (AIAG-VDA FMEA Handbook 2019), often moves away from simple RPN multiplication in favor of Action Priority tables that take into account various combinations of S, O, D without arithmetic manipulations.
CONCLUSIONS
Contributors:
Semchenko K.V. – writing – original draft, supervision;
Iakovenko V.K. – methodology, writing – review and editing;
Shmalko O.O. – conceptualization, methodology – review and editing;
Oliinyk S.V. – conceptualization, writing – review and editing.
Funding. The research was conducted under the financing from the funds of National University of Pharmacy at the topic ща initiative direction “Development of composition, technology and biopharmaceutical research of medicines based on natural and synthetic raw materials” (state registration number: 0114U000945).
Conflict of interests. The authors declare that they have no conflict of interest in relation to this research, whether financial, personal, authorship or otherwise, that could affect the research and its results presented in this paper.
REFERENCES
Ключові слова: патентна монополія, «вічнозелені» патенти, лікарські засоби, зловживання патентними правами, конкуренція, інтелектуальна власність
Key words: patent monopoly, “evergreen” patents medicines, patent abuse, competition, intellectual property
Реферат
У статті здійснено систематизований аналіз наукових публікацій, присвячених сучасним тенденціям зловживання патентними правами у фармацевтичній галузі США, зокрема механізмам реалізації стратегій «вічнозелених» патентів та їх економіко-правовим наслідкам. Метою роботи було проведення систематизованого огляду наукової літератури щодо тенденцій зловживання патентними правами у фармацевтичному секторі США, з акцентом на механізмах реалізації стратегій «вічнозелених» патентів, їх економіко-правових наслідках та можливих напрямах удосконалення регуляторної політики. Для досягнення поставленої мети було застосовано методологію систематичного огляду літератури відповідно до рекомендацій PRISMA, у поєднанні із загальнонауковими та спеціальними методами наукового пізнання: системно-структурний, діалектичний, формально-логічний, порівняльно-правовий, методи аналізу та синтезу. Використання цих методів дозволило оцінити сучасний стан патентного регулювання в США, ідентифікувати правові інструменти продовження патентної монополії та проаналізувати їх вплив на доступність генеричних та/або біосимілярних препаратів. Матеріальною базою дослідження стали наукові публікації, аналітичні та статистичні звіти (PubMed, JAMA, Scopus, Springer, BMC, Oxford Academic), звіти та прогнози міжнародних організацій (DrugPatentWatch, ProClinical, PhRMA, Statista), а також офіційні документи Управління з патентів і торговельних марок США (USPTO), Угоди TRIPS та законодавство США у сфері патентного права (U.S. Patent Act, Hatch–Waxman Act). Із 286 ідентифікованих публікацій до якісного аналізу було включено 40 джерел, за період 2008–2025 років. Критеріями включення були джерела, що містять дані про патентний захист лікарських засобів, стратегії «вічнозелених» патентів, економічні наслідки та доступність медичних технологій. Джерела без прямого відношення до теми дослідження або з недостатньою науковою достовірністю виключалися. За результатами дослідження засвідчено, що фармацевтичні компанії США системно застосовують багаторівневі патентні стратегії, спрямовані на пролонгацію ринкової ексклюзивності після завершення базового патентного строку, підвищення цін на лікарські засоби та обмеження доступності терапії для споживачів. Водночас емпіричними даними підтверджено, що завершення строку дії патентів створює умови для активізації ринкової конкуренції та зниження цін на генерики на 30-50% протягом перших років. Підкреслено необхідність удосконалення регуляторних механізмів патентного законодавства США, включаючи обмеження практик «вічнозелених» патентів та забезпечення прозорості ринкових процесів. Надано прогноз щодо структурних змін у фармацевтичному ринку США в період 2025-2029 років, пов’язаних із завершенням строків дії ключових патентів на оригінальні лікарські засоби, а також запропоновано шляхи досягнення балансу між інтересами інноваційного розвитку та суспільними потребами в доступних лікарських засобах.
Abstract
Trends in the abuse of patent rights for medicinal products in the United States (review). Kodynets A.O., Doroshenko O.F., Volynets I.P., Dorozhko G.K., Petrenko V.O., Fedorova N.V. The article provides a systematic analysis of scholarly publications addressing contemporary trends in the abuse of patent rights in the pharmaceutical sector of the United States, with particular emphasis on the mechanisms for implementing “evergreen” patent strategies and their economic and legal consequences. The purpose of the study was to conduct a systematic review of the scientific literature on trends in the abuse of patent rights in the U.S. pharmaceutical sector, focusing on the mechanisms of “evergreen” patent strategies, their economic and legal implications, and possible directions for improving regulatory policy. To achieve this objective, a systematic literature review methodology was applied in accordance with the PRISMA guidelines, in combination with general scientific and special research methods, including the systemic-structural, dialectical, formal-logical, and comparative legal approaches, as well as methods of analysis and synthesis. The use of these methods made it possible to assess the current state of patent regulation in the United States, identify legal instruments for extending patent monopolies, and analyze their impact on the availability of generic and/or biosimilar medicines. The empirical basis of the study consisted of scientific publications, analytical and statistical reports indexed in PubMed, JAMA, Scopus, Springer, BMC, and Oxford Academic, reports and forecasts of international organizations (DrugPatentWatch, ProClinical, PhRMA, Statista), as well as official documents of the United States Patent and Trademark Office (USPTO), the TRIPS Agreement, and U.S. patent legislation (the U.S. Patent Act and the Hatch–Waxman Act). Out of 286 identified publications, 40 sources published between 2008 and 2025 were included in the qualitative analysis. Inclusion criteria comprised sources containing data on pharmaceutical patent protection, “evergreen” patent strategies, economic consequences, and access to medical technologies. Sources lacking a direct connection to the subject of the study or failing to meet scientific reliability standards were excluded. The results of the study demonstrate that U.S. pharmaceutical companies systematically employ multi-layered patent strategies aimed at prolonging market exclusivity beyond the expiration of the basic patent term, increasing drug prices, and restricting access to therapy for consumers. At the same time, empirical evidence confirms that patent expiration creates conditions for intensified market competition and a reduction in generic drug prices by 30–50% within the first years following market entry. The study emphasizes the need to improve regulatory mechanisms within U.S. patent law, including limiting “evergreen” practices and ensuring greater transparency of market processes. A forecast of structural changes in the U.S. pharmaceutical market for the period 2025-2029 is provided, associated with the expiration of key patents for original medicines, and approaches are proposed to achieve a balance between the interests of innovative development and societal needs for affordable medicines.
Інтелектуальна власність у фармацевтичній галузі виступає ключовим інструментом стимулювання інноваційної активності, забезпечення відтворюваності науково-дослідного циклу та збереження конкурентоспроможності на ринку. Як зазначають R.A. Pires, J.J. Ferreira, патентні механізми у сфері фармацевтики відіграють системоутворювальну роль в поєднанні стратегій інноваційного розвитку та інтелектуальної власності, створюючи своєрідний баланс між суспільними інтересами та приватними інвестиціями [26]. Патентний захист лікарських засобів (далі також – препарати/ ліки) традиційно обґрунтовується необхідністю компенсації значних фінансових витрат і тривалих клінічних досліджень, які супроводжують створення нових препаратів.
За оцінками аналітичних звітів DrugPatentWatch, середня вартість розроблення інноваційного лікарського засобу – від початкових лабораторних досліджень до впровадження продукту на ринок – становить близько 2,3 млрд дол. США, тоді як залежно від фармакологічної групи, технологічної складності та терапевтичного спрямування цей показник може коливатися в діапазоні від 300 млн до 4,5 млрд дол. США [39].
Водночас протягом останніх десятиліть спостерігається стійка тенденція використання патентних механізмів не лише як засобу стимулювання інновацій, але і як інструменту подовження монопольного контролю над фармацевтичним ринком. У науковій літературі таку стратегію позначають терміном «evergreening», або «вічнозелені» патенти, що передбачає створення багатошарових патентних портфелів, спрямованих на ускладнення або відтермінування доступу генеричних та/або біосимілярних лікарських засобів [1, 15].
Дослідження свідчать, що тенденція у фармацевтичній галузі полягає в зростанні кількості патентних заявок на незначні модифікації вже наявних препаратів – зміну рецептури, солі, ізомерів, поліморфів чи комбінування відомих лікарських сполук. При цьому кількість дійсно нових хімічних субстанцій, що впроваджуються у фармацевтичну практику, залишається стабільно низькою, демонструючи тенденцію до скорочення [3]. Таке зміщення акцентів з розроблення принципово нових активних речовин на мінімально модифіковані варіанти вже наявних молекул свідчить про інституціоналізацію стратегій «вічнозелених» патентів як поширеного бізнес-інструменту підтримання ринкової ексклюзивності.
Вказані стратегії зумовлюють низку економіко-правових наслідків, зокрема підвищення вартості лікування, зниження доступності життєво необхідних препаратів, уповільнення розвитку ринку генериків та зростання фінансового навантаження на системи охорони здоров’я. Означені процеси набувають особливої актуальності в умовах глобального зростання попиту на інноваційні лікарські засоби.
Мета дослідження полягає у проведенні систематизованого огляду наукової літератури щодо тенденцій зловживання патентними правами у фармацевтичному секторі США, з акцентом на механізмах реалізації стратегій «вічнозелених» патентів, їх економіко-правових наслідках та можливих напрямах удосконалення регуляторної політики.
МАТЕРІАЛИ ТА МЕТОДИ ДОСЛІДЖЕНЬ
Основою методологічного інструментарію дослідження стали загальнонаукові та спеціальні методи наукового пізнання: системно-структурний, діалектичний, формально-логічний, порівняльно-правовий, а також методи аналізу та синтезу. Вони забезпечили комплексний підхід до вивчення сучасних тенденцій зловживання патентними правами у фармацевтичному секторі США та визначення можливих напрямів удосконалення регуляторної політики.
Зокрема, порівняльно-правовий метод застосовувався для аналізу законодавчого регулювання патентного захисту лікарських засобів у США, а також для виявлення механізмів реалізації стратегій «вічнозелених» патентів і їх впливу на доступність лікарських засобів. Системно-структурний метод використовувався при оцінюванні структури фармацевтичного ринку, динаміки продажів оригінальних та генеричних препаратів, а також побудові прогнозів зміни цінової політики після завершення строку дії патентів. Методи аналізу та синтезу дозволили узагальнити наявні емпіричні та теоретичні дані щодо економічних та соціальних наслідків застосування стратегій «вічнозелених» патентів.
В основу дослідження увійшли матеріали з відкритих джерел, наукові публікації, статистичні та аналітичні звіти, нормативно-правові акти та міжнародні документи. Зокрема було проаналізовано матеріали з баз даних і пошукових систем (PubMed, JAMA, Scopus, Springer, BMC, Oxford Academic), звіти та прогнози міжнародних організацій (DrugPatentWatch, ProClinical, PhRMA, Statista), а також офіційні документи Управління з патентів і торговельних марок США (USPTO), Угоди TRIPS та законодавство США у сфері патентного права (U.S. Patent Act, Hatch–Waxman Act).
Теоретичною базою дослідження стали праці науковців та практиків різних галузей науки, зокрема у сфері фармацевтики та інтелектуальної власності, серед яких A. Kodynets, O. Doroshenko, I. Volynets, G. Dorozhko, V. Petrenko, V. Belitsky [1], S. Adepu, S. Ramakrishna [5], R. Aryan [7], M. Boldrin, D. Levine [8], H. Burke [9], G. Dwivedi, S. Hallihosur, L. Rangan [11], F. Gaessler, S. Wagner [12], L. Gorman [13], O. Granstrand, F. Tietze [14, 15]; C. Hemphill, B. Sampat [17, 18], M. Janczura, S. Sip, J. Cielecka-Piontek [20], S. Kolia [22], S. Myles [23], R. Pires, J. Ferreira [26], G. Quinn [27], P. Upadhyaya [35], V. Uyen [36], A. Vahrenwald, G. Pedde [37], F. Waller [38] та інші. Зокрема доповнимо, що роботи M. Boldrin, D. Levine, C. Hemphill, B. Sampat аналізують економічні ефекти патентної монополії; дослідження A. Kodynets, O. Doroshenko, I. Volynets та ін. розкривають правові аспекти патентного регулювання у фармацевтичній сфері; праці G. Quinn, O. Granstrand, F. Tietze присвячені інноваційним стратегіям фармацевтичних корпорацій та механізмам захисту інтелектуальної власності. Проте, незважаючи на наявність значної кількості досліджень, окремі аспекти тенденції зловживання патентними правами на лікарські засоби в США потребують подальшого вивчення.
Дослідження проведено у формі систематичного огляду літератури відповідно до рекомендацій PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). Пошук джерел здійснювався у вищезазначених базах даних PubMed, Scopus, Web of Science, SpringerLink, Oxford Academic та інших відкритих джерелах за період 2008-2025 років з використанням ключових слів: pharmaceutical patents, evergreening strategies, patent abuse, generic drugs, Hatch-Waxman Act.
У результаті первинного пошуку ідентифіковано 286 джерел. Після видалення дублікатів (n=74) та скринінгу за назвами й анотаціями (n=212) було виключено 142 джерела, що не відповідали тематиці дослідження. Повнотекстовий аналіз проведено для 70 публікацій, з яких 30 було виключено через відсутність прямого зв’язку з патентним регулюванням або недостатню достовірність. У підсумку до якісного аналізу включено 40 джерел. Критеріями включення слугували наукові статті, аналітичні огляди, статистичні звіти, нормативно-правові акти та офіційні документи, що стосуються патентного захисту лікарських засобів, стратегій «вічнозелених» патентів та економічних наслідків їх застосування. Критеріями виключення стали джерела, що не містили прямого зв’язку з патентним регулюванням фармацевтичної галузі або не відповідали вимогам наукової верифікованості.
Особлива увага приділялась аналізу патентних стратегій найбільших фармацевтичних корпорацій, наслідків завершення строків дії патентів та моделей виходу на ринок генеричних та/або біосимілярних препаратів. Для систематизації даних було складено таблицю щодо строків дії патентів на оригінальні лікарські засоби, обсяги продажів та стратегії компаній щодо продовження ринкової ексклюзивності.
РЕЗУЛЬТАТИ ТА ЇХ ОБГОВОРЕННЯ
Фармацевтичні патенти становлять наріжний камінь сучасної інноваційної екосистеми, оскільки саме вони створюють ключові стимули для фармацевтичних компаній інвестувати у складний, тривалий та фінансово витратний процес розробки нових лікарських засобів. Як зазначає дослідження PhRMA, середній цикл створення й виведення на ринок одного фармацевтичного продукту триває понад десять років і вимагає близько 2,6 мільярда доларів інвестицій від моменту відкриття активної речовини до отримання схвалення регуляторних органів [28].
В умовах відсутності патентного захисту компанії не мали б можливості компенсувати витрати на розробку, оскільки конкуренти могли б швидко відтворити новий препарат і реалізовувати його у вигляді генерика за значно нижчою ціною. Патенти, надаючи тимчасову монополію (зазвичай протягом 20 років з дати подання заявки), забезпечують власникові виключне право на комерційне використання винаходу. Вбачаємо, що правова ексклюзивність дає змогу фармацевтичним компаніям встановлювати ціни, які враховують не лише фактичні витрати на дослідження й розробки, а й високі ризики невдач, адже більшість потенційних лікарських засобів не проходять клінічні випробування. Як наголошують F. Gaessler, S.Wagner, отриманий у результаті комерціалізації прибуток виконує подвійну функцію: по-перше, фінансує майбутні інновації, а по-друге, компенсує значний рівень відтоку ресурсів у процесі фармацевтичних досліджень [12].
Водночас патентна система у фармацевтичній галузі не позбавлена критики. Науковці звертають увагу, що патенти можуть призводити до надмірного зростання цін на лікарські засоби, обмежуючи доступ до необхідних медикаментів, особливо в країнах з низьким і середнім рівнем доходу. Як підкреслюють A. Vahrenwald, G. Pedde, випадки високої вартості ліків для лікування рідкісних (орфанних) хвороб демонструють напруження між необхідністю забезпечення стимулів для інновацій та суспільним обов’язком гарантувати доступність медичних технологій для всіх верств населення [37].
З аналогічних позицій виступають M. Boldrin, D. Levine, які у своїй фундаментальній праці «Against Intellectual Monopoly» стверджують, що надмірна монополізація інтелектуальної власності може, навпаки, гальмувати інноваційні процеси. На думку авторів, надлишковий патентний захист у фармацевтичній сфері формує бар’єри для конкуренції та обмежує потенціал подальших наукових відкриттів, зменшуючи загальну ефективність інноваційної системи [8].
Таким чином, хоча патентний механізм залишається основним інструментом підтримки інновацій у фармацевтичному секторі, його ефективність залежить від збалансованості між приватними економічними інтересами та суспільними цілями, зокрема забезпеченням доступності лікарських засобів і зниженням вартості лікування для споживачів.
Система патентного права США традиційно вважається однією з найбільш сприятливих для власників фармацевтичних патентів. Вона функціонує на основі положень Закону США «Про патенти» (U.S. Patent Act) [33] та тлумачиться в контексті положень Угоди про торговельні аспекти прав інтелектуальної власності (TRIPS, 1994) [6], ухваленої в межах Світової організації торгівлі (WTO), а також адміністративної практики Відомства з патентів і торговельних марок США (USPTO) [24]. Така правова архітектура створює передумови для формування багаторівневої системи охорони одного й того самого лікарського засобу, що забезпечує тривале збереження ринкової ексклюзивності інноваційних препаратів [7, 40].
Ухвалення в 1984 році Закону Хетча–Ваксмана (Hatch-Waxman Act) було спрямоване на стимулювання виходу на ринок генеричних лікарських засобів, проте водночас надало фармацевтичним компаніям-виробникам оригінальних препаратів низку правових механізмів для пролонгації строку дії патентної охорони [16, 18]. До таких інструментів належать подання нових заявок на патенти, що стосуються модифікованих версій уже наявних препаратів (зміни у складі, дозуванні, способі доставки активної речовини тощо), можливість ініціювання 30-місячних відстрочок розгляду заявок на генерики в межах судових процесів, що подаються відповідно до пункту IV Закону Хетча-Ваксмана [7].
Подібна правова модель піддається критиці з боку науковців та експертів фармацевтичного ринку, оскільки створює умови для формування так званих «патентних чагарників» (patent thickets) – складних мереж взаємопов’язаних патентів, які суттєво ускладнюють вихід генеричних аналогів на ринок [30, 34, 7].
Великі транснаціональні фармацевтичні корпорації формують розгалужені патентні портфелі, що охоплюють тисячі об’єктів інтелектуальної власності та забезпечують комплексний правовий захист розроблених ними лікарських засобів. Така стратегія дозволяє не лише зберігати домінуючі позиції на світовому ринку, але й ефективно контролювати доступ конкурентів до виробництва генеричних аналогів. Як зазначають A. Vahrenwald, G. Pedde, ключові фармацевтичні компанії – Pfizer, Merck & Co., Johnson & Johnson та інші – інвестують мільярди доларів у дослідження та розробки, отримуючи при цьому значні прибутки від комерціалізації своїх інноваційних препаратів [37].
На переконання A. Vahrenwald, G. Pedde, подібна багаторівнева патентна стратегія не лише зміцнює ринкові позиції фармацевтичних гігантів, а й утруднює вихід генеричних компаній на ринок після завершення первинного строку дії патенту. У результаті формується своєрідна «патентна фортеця», яка фактично продовжує комерційну монополію оригінатора і впливає на динаміку цін та доступність лікарських засобів для споживачів [37].
Закінчення строку дії патентного захисту є критичним етапом життєвого циклу будь-якого фармацевтичного продукту, оскільки саме воно знаменує перехід від монопольного ціноутворення до умов відкритої ринкової конкуренції. Цей процес, відомий як втрата виключних прав, зазвичай відкриває шлях для виходу на ринок генеричних та/або біосимілярних препаратів, що суттєво змінює цінову динаміку та структуру прибутків у фармацевтичній галузі.
Дослідження L. Gorman демонструє, що після завершення строку дії патенту середня ціна на рецептурні лікарські засоби знижується в межах 38-48%, що зумовлено активізацією конкуренції з боку виробників генериків [13]. Така тенденція вказує на тісний зв’язок між режимом патентного захисту та рівнем доступності лікарських засобів для споживачів.
Більш масштабне міжнародне дослідження, проведене M. Serra-Burriel, N. Martin-Bassols, G. Perényi, охоплювало 505 препаратів, термін дії патентів на які закінчувався у восьми країнах – Австралії, Канаді, Франції, Німеччині, Японії, Швейцарії, Великій Британії та США. Автори встановили, що зниження цін після завершення дії патенту було статистично значущим упродовж восьмирічного періоду, причому найінтенсивніше падіння спостерігалося саме в США: у перший рік після втрати патентного захисту ціни зменшувалися на 32% (95% ДІ, 24-39%), а протягом восьми років – на 82% (95% ДІ, 71-89%) [10].
Крім того, результати економічного моделювання, проведеного цими авторами, показали, що неврахування виходу генериків на ринок може призводити до упереджених показників економічної ефективності лікарських засобів – від +40% до -40%, залежно від заданого сценарію. Показово, що врахування етапу втрати виключних прав є необхідним елементом оцінки вартості медичних технологій і має бути системно інтегрованим у процес ухвалення рішень у сфері охорони здоров’я.
У найближчій перспективі світовий фармацевтичний ринок очікує на масове завершення строків дії патентного захисту низки найбільш прибуткових лікарських засобів. Протягом 2025-2029 років спливання терміну ключових патентів на такі продукти зумовить глибокі структурні зміни в конкурентному середовищі галузі [9]. Зі свого боку, матиме комплексний вплив на стратегії інноваційного розвитку фармацевтичних корпорацій, інвестиційну активність, а також цінову політику та динаміку ринкових консолідацій у форматі злиттів і поглинань.
Втрати патентного захисту змушують виробників оригінальних препаратів адаптувати бізнес-моделі, орієнтуючись на диверсифікацію портфелів, виведення модифікованих форм препаратів (нових солей, ізомерів, комбінацій активних речовин) або перехід до біотехнологічних рішень і персоналізованої медицини. Одночасно активізуються процеси зміцнення позицій на зростаючих ринках через стратегічні партнерства, угоди з виробниками генериків та «вічнозелених» патентів, спрямовані на пролонгацію періоду ринкової ексклюзивності.
У таблиці наведено вибірку найприбутковіших оригінальних лікарських засобів, строки дії патентів на які спливають у період 2025-2029 років [9, 22], із зазначенням компаній-виробників, основних терапевтичних показань, а також типових стратегій реагування на втрату патентного захисту.
Назва лікарського засобу Компанія Рік (роки) закінчення патенту Основне призначення Обсяг продажу на прикладі 2023 р. Стратегія компанії EYLEA Regeneron / Bayer 2025–2026 Вікова макулодистрофія, діабетична ретинопатія 5,9 млрд дол. США (США) Диверсифікація доходів, розробка нових молекул PROLIA/XGEVA (Denosumab) Amgen 2025–2026 Метастази в кістки, остеопороз +9% річного зростання у 2023 р. Фокус на науково-дослідних та дослідно-конструкторських роботах (НДДКР) в онкології та імунології PREVNAR 13 Pfizer 2026 Вакцина проти пневмококу Багатомільярдні продажі з 2010 р. Масштабні інвестиції в НДДКР та придбання Seagen Inc. XARELTO (Rivaroxaban) Bayer / Johnson & Johnson 2026 Антикоагулянт, профілактика тромбозів €4,5 млрд (2022), понад 80 млн рецептів у США Розвиток напрямів генної та клітинної терапії IBRANCE (Palbociclib) Pfizer 2027 Рак молочної залози (HR+/HER2–) Зниження продажів на 13% у 2023 р. Розширення онкопортфеля (Array BioPharma, Seagen) TRULICITY (Dulaglutide) Eli Lilly 2027 Цукровий діабет II типу 17-й за обсягами продажів у світі (2023 р.) Перехід на препарат нового покоління Mounjaro ELIQUIS (Apixaban) Bristol Myers Squibb / Pfizer 2027–2029 Профілактика тромбозів Один з лідерів у своєму класі Судовий захист патенту, дитяча ексклюзивність KEYTRUDA (Pembrolizumab) Merck & Co. 2028 Імунотерапія раку (меланома, легені, лімфома тощо) $33,7 млрд (прогноз на 2028 р.) Розширення портфеля онкопрепаратів, придбання Harpoon Therapeutics OPDIVO (Nivolumab) Bristol Myers Squibb 2028 Імунотерапія раку $9,0 млрд (2023 р.) Розробка шести нових препаратів для компенсації втрат OCREVUS (Ocrelizumab) Roche 2028–2029 Розсіяний склероз CHF 6,38 млрд (2023 р.) Інвестиції в дослідження раку молочної залози та кардіометаболічних хворобТаблиця. Строки дії патентів на оригінальні лікарські засоби, які спливають у 2025-2029рр. ↓
(торговельна марка)
(ДВТ, ТЕЛА)
Наведені дані демонструють, що перехід до постпатентної фази для більшості компаній супроводжується переглядом інноваційних пріоритетів і посиленням конкуренції з боку виробників генеричних та/або біосимілярних препаратів.
Відтак патентна система у фармацевтичній сфері виконує подвійну функцію: з одного боку, вона стимулює НДДКР, формуючи економічні стимули для розроблення інноваційних лікарських засобів; з іншого – забезпечує механізм економічної віддачі від інновацій, що підтримує сталий розвиток галузі [5].
Разом з тим, на тлі зростання вартості досліджень і посилення конкуренції, спостерігається поширення практик «вічнозеленого» патентування – стратегії, спрямованої на продовження комерційної виключності лікарських засобів понад початковий строк дії базового патенту. Сутність цієї стратегії полягає в системному отриманні додаткових патентів на незначні модифікації, поступові вдосконалення або нові способи застосування вже відомих препаратів [29, 31].
Хоча деякі з таких удосконалень можуть мати клінічну значущість (наприклад, покращення біодоступності чи зручності застосування), у більшості випадків вони використовуються як інструмент пролонгації ринкової монополії без суттєвого наукового прориву [5, 29, 31].
Показовим прикладом є препарат Phesgo (підшкірна комбінація трастузумабу та пертузумабу), схвалений у 2020 році. Завдяки зручнішому способу введення він швидко витіснив внутрішньовенні форми, для яких уже існували біосиміляри, фактично нівелюючи очікуваний ефект конкуренції. Інший приклад – Lytenava (внутрішньоочна форма бевацизумабу), який отримав статус нового оригінатора та власний патентний і регуляторний захист, попри завершення охорони базової форми Avastin [32].
У науковій літературі [22] та патентно-аналітичних звітах виокремлюють кілька найпоширеніших форм прояву стратегій «вічнозелених» патентів: нові форми та способи дозування, нові методи застосування або показання, патентування поліморфів й ізомерів, комбіновані лікарські форми [5, 22, 29, 20, 31]. Узагальнений перелік похідних речовин, з яких отримують «вічнозелений» патент, включає: фармацевтичні форми відомої хімічної сполуки; комбінації декількох активних речовин, які є відомими хімічними сполуками; солі, складні та прості ефіри відомих хімічних сполук; поліморфи; оптичні ізомери (енантіомери) відомих хімічних сполук; сполуки за формулою Маркуша; селекційні винаходи; проліки; метаболіти [2, 4].
Питання «вічнозелених» патентів є предметом гострих наукових і суспільних дискусій. Прихильники цієї стратегії розглядають її як один із механізмів підтримання інноваційної динаміки фармацевтичної галузі, стверджуючи, що інкрементальні вдосконалення лікарських засобів сприяють підвищенню їхньої якості, безпечності та зручності застосування для пацієнтів. Водночас критики наголошують, що стратегії «вічнозелених» патентів уповільнюють конкуренцію, призводять до підвищення цін на лікарські засоби та обмежують доступ до більш доступних генеричних препаратів [14, 36]. Попри широку критику, «вічнозелене» патентування залишається типовою стратегічною відповіддю інноваційних компаній на економічні виклики, пов’язані з високими витратами на дослідження та коротким періодом ефективної патентної охорони. Як зазначає O. Granstrand [14], фінансовий тиск, спричинений необхідністю максимізувати прибутки протягом обмеженого «вікна ексклюзивності», формує замкнене коло: високі витрати на НДДКР → впровадження «вічнозелених» патентів → зростання кількості патентних спорів і формування «патентних чагарників» → затримка виходу генериків → підвищення кінцевих цін для споживачів.
Вищезазначену тенденцію підтверджують сучасні аналітичні дані. Дослідження організації I-MAK демонструє системність патентних практик, спрямованих на тривале збереження ринкової ексклюзивності. Так, препарат Humira (AbbVie), призначений для лікування ревматоїдного артриту, має 311 патентних заявок, з яких 165 надано охорону, що забезпечило понад 43 роки монопольного контролю. Препарат Keytruda (Merck), розроблений для онкологічних показань, має 180 заявок, з яких 78 чинні, що гарантує близько 37 років ексклюзивності. Аналогічно, Enbrel (Amgen) перебуватиме під патентним захистом майже 50 років, що у 2,5 раза перевищує базовий 20-річний строк [19; 25].
Отже, дискусія в сучасному науковому та регуляторному середовищі вже не стосується питання, чи застосовуватимуть фармацевтичні компанії стратегії «вічнозелених» патентів, а радше – яким чином можна досягти балансу між комерційною необхідністю підтримання інновацій та суспільним інтересом у забезпеченні доступності лікарських засобів.
Як зазначають закордонні експерти, зокрема F.J. Waller, патенти є допоміжним інструментом захисту для нових підприємств, тобто патенти не дають можливість іншим фармацевтичним компаніям користуватися новими технологіями, які на момент виникнення є передовими та сучасними. Водночас компанія-винахідник може збагатитись за рахунок видачі ліцензій і отримання роялті [38].
Окремі проблемні питання щодо патентування лікарських засобів відзначила Н. Г. Медведева, яка виявила, що дотепер перед розробниками лікарського засобу постає складний вибір: чи патентувати нову хімічну сполуку або породжувати «вічнозелений» патент, зокрема через відсутність рекомендацій щодо опису родових структур або структур Маркуша [2, 23, 35].
Ще однією відомою структурою, яку використовують американські винахідники, є формула винаходу Джепсона (Jepson claim), за якою у вступній частині описується рівень техніки, а в заключній – елементи новизни, пропоновані заявником [21]. G. Quinn категорично проти зазначеної структури в заявках, через те, що, по-перше, законодавство США і так дозволяє охороняти винаходи, які є удосконаленнями роботи інших (35 U.S. Code § 101. Inventions patentable), тобто не є новаторськими, а по-друге, відповідна формула дозволяє патентовласникові використовувати преамбулу для викладу елементів або етапів заявленого винаходу, що є загальноприйнятими або відомими, тим самим користь від нового винаходу є мінімальна [27].
Вартує уваги, на наш погляд, наукова праця вчених G. Dwivedi, S. Hallihosur, L. Rangan щодо «оновлення» як імітації (обману), яке використовується в патентному праві. Зокрема, автори наголосили, що хоча «вічнозелений» патент не є офіційно-правовим поняттям, він позначає численні способи патентовласників фармацевтичної продукції за допомогою патентних законів розширити свої монопольні привілеї на строки, які зазвичай дозволяються та визначені відповідними нормативно-правовими актами, особливо щодо лікарських засобів з високим рівнем прибутку [11]. Мається на увазі те, що фармацевтичні компанії зловживають патентною системою на власну користь та видозмінюють вже наявні лікарські засоби, випускаючи їх в обіг як нові. У такий спосіб, отримуючи новий патент на оригінальний лікарський засіб, виробники навмисно обмежують випуск генеричних версій, запобігаючи виникнення конкуренції. Тому відповідна стратегія є недобросовісною.
Ефект, на який розраховують фармацевтичні компанії від власних дій, направлених на отримання «вічнозеленого» патенту, – це довготривале збереження ексклюзивності даних оригінального лікарського засобу, утримання монополії, а також максимізація прибутків від продажу [11]. Проте для споживачів масштабований випуск дороговартістних лікарських засобів, так званих «блокбастерів», не покращить здоров’я, а навпаки – чим дорожчий товар, тим менше можливості його придбати (особливо для третіх країн). Натомість очікуваний дохід від прибутків з часом може досягнути свого плато.
Ще одна робота C. Hemphill, B. Sampat свідчить про наявність іншої проблематики у створенні «вічнозелених» патентів. Зокрема, проведене дослідження підтверджує, що штучне продовження патентного захисту спричиняє виникнення патентів низької якості (lower quality patents) через збереження патентів на лікарські засоби, термін дії яких спливає. У перспективі, за висновками авторів, відбудеться стрімке усунення генеричних версій лікарських засобів, що може позначитись на здоров’ї населення по всьому світу [17].
Таким чином, результати систематичного огляду показали, що в США сформувалася інституціоналізована модель багаторівневого патентного захисту фармацевтичних інновацій, яка дозволяє компаніям пролонгувати ринкову ексклюзивність далеко за межі базового 20-річного строку. Аналіз відібраних джерел підтвердив, що стратегії «evergreening» є поширеною корпоративною практикою, яка реалізується через патентування нових форм, способів дозування, комбінацій активних речовин, ізомерів, поліморфів та нових показань. Емпіричні дані одностайно свідчать, що завершення строку дії патентів супроводжується істотним зниженням цін на лікарські засоби, що підтверджує безпосередній вплив патентного режиму на доступність лікування.
ВИСНОВКИ
Внески авторів:
Кодинець А.О. – концептуалізація, ведення, написання – рецензування та редагування, візуалізація, перевірка;
Дорошенко О.Ф. – ведення, редагування, формальний аналіз, перевірка;
Волинець І.П. – дослідження, методологія, курація даних, написання – початковий проєкт;
Дорожко Г.К. – формальний аналіз, ведення, перевірка;
Петренко В.О. – адміністрування проєкту, редагування, підготовка роботи до друку;
Федорова Н.В. – ведення, перевірка.
Фінансування. Дослідження не має зовнішніх джерел фінансування.
Конфлікт інтересів. Автори заявляють про відсутність конфлікту інтересів.
REFERENCES
Key words: tennis, athlete, nutrition, performance
Ключові слова: теніс, спортсмен, харчування, продуктивність
Abstract
Nutrition is crucial in improving athlete performance, and research on the relationship between nutrition and sport continues to grow. This article aims to investigate nutrition's influence on tennis athletes' performance through a systematic review approach. The main objective was to identify the types of food that are most influential in improving the performance of tennis athletes, as well as to evaluate their impact on physiological and psychological aspects. This study used a systematic review approach, following PRISMA guidelines. Databases such as PubMed, Scopus, and Web of Science were reviewed for articles published up to 2024, using keywords related to nutrition and tennis. Inclusion and exclusion criteria were set to select articles that fit the research topic. Data were then extracted, synthesized, and analyzed to produce significant findings in the context of nutrition's influence on tennis athletes' performance. Of the 500 articles identified, 44 met the inclusion criteria. The analysis concluded that nutrition is essential in enhancing a tennis athlete's performance. Carbohydrates, protein, and fat were shown to be vital sources of energy for tennis athletes, while vitamins and minerals play an essential role in recovery and optimal body function. Previous studies have also shown that proper diet and supplementation can significantly improve tennis athletes' stamina, strength, and recovery. This study confirms that proper nutrition is highly influential in improving the performance of tennis athletes. Optimizing carbohydrate, protein, fat, vitamin, and mineral intake can have significant physiological and psychological benefits such as stamina, strength, and recovery. These findings result in recommendations for a tennis athlete's diet tailored to individual needs. At the same time, further research is recommended to deepen the understanding of the relationship between nutrition and sports performance.
Реферат
Вплив харчування на результативність тенісистів: систематичний огляд. Саюти Йогі, Сабіллах Мухамад Іхсан, Хідаят Резга Аржан, Шоліхах Іма Фітрі. Харчування відіграє вирішальну роль у підвищенні спортивної результативності спортсменів, й інтерес до вивчення взаємозв’язку між харчуванням і спортивними досягненнями продовжує зростати. Метою цієї статті є дослідити вплив харчування на результативність тенісистів за допомогою методу систематичного огляду. Основним завданням є визначення типів харчування, які мають найбільший вплив на спортивні показники, а також оцінювання їхнього впливу на фізіологічні та психологічні аспекти підготовки тенісистів. Дослідження проведено відповідно до методології PRISMA. Було проаналізовано наукові бази даних, зокрема PubMed, Scopus і Web of Science, з використанням ключових слів, пов’язаних із харчуванням і тенісом, для виявлення публікацій до 2024 року. Встановлено чіткі критерії включення та виключення для відбору релевантних статей. Відібрані дані були систематизовані, синтезовані та проаналізовані з метою формулювання обґрунтованих висновків щодо впливу харчування на спортивні результати. З 500 проаналізованих публікацій 44 відповідали критеріям включення. Результати аналізу підтверджують, що харчування має суттєвий вплив на спортивну результативність тенісистів. Встановлено, що вуглеводи, білки та жири є ключовими джерелами енергії, а вітаміни й мінерали відіграють важливу роль у відновленні та підтримці оптимального функціонування організму. Попередні дослідження також засвідчили, що збалансоване харчування і відповідні добавки значно покращують витривалість, силу та процес відновлення. Таким чином, результати цього огляду підтверджують важливість правильного харчування для підвищення спортивної ефективності тенісистів. Оптимізація споживання макро- й мікроелементів може забезпечити значні фізіологічні та психологічні переваги. На основі отриманих даних сформульовано рекомендації щодо розробки індивідуальних програм харчування для тенісистів. У майбутньому доцільно проводити додаткові дослідження з метою глибшого вивчення впливу харчування на спортивні досягнення.
Nutrition is one of the critical factors that influence athletic performance. A proper diet is vital, particularly in competitive sports such as tennis, where energy and recovery requirements are high. Tennis requires a combination of strength, endurance, speed, and agility, thus requiring comprehensive nutritional support to support all these physical aspects [1]. Proper dietary choices increase energy during play, speed up recovery, reduce the risk of injury, and maximize physiological function during matches that last several hours. Correspondingly, research in sports nutrition continues to grow, focusing on how nutrition can be optimized to support athlete performance. Studies have shown that a balanced intake of carbohydrates, protein, and fat is essential in supporting intense and prolonged physical activities, such as those often encountered in tennis [2]. Further research also indicates the importance of micronutrients, such as vitamins and minerals, which are crucial in maintaining athlete health and optimizing performance [3].
This systematic review investigates and analyzes the literature on nutrition's influence on tennis athlete performance. Through in-depth analysis, it aims to identify the nutritional components that are most influential in improving performance and provide recommendations that athletes and coaches can use in designing effective dietary programs. This review will answer the following research questions: What types of nutrition are most effective in improving the performance of tennis athletes, and how do they affect athletes' physiological and psychological aspects during competition? This review hopes to fill a gap in the literature by systematically collecting and synthesizing existing data, which will provide evidence-based guidance in sports nutrition, particularly tennis. According to [4], adequate carbohydrate intake before and during tennis play can significantly improve performance, reduce fatigue, and increase concentration during play. Research [5] supports these findings, stating that protein is crucial for post-match muscle recovery and muscle protein synthesis during high-intensity exercise. This unity in the literature suggests that a combination of carbohydrates and protein is key in the diet of tennis athletes.
Therefore, through this systematic review, we will delve deeper into nutrition's influence on tennis athletes' performance, hoping to provide new insights and valuable global recommendations for the tennis community. With a better understanding of the relationship between nutrition and performance, athletes and coaches can be better guided in setting more effective and efficient nutritional strategies to achieve optimal results on the court.
Review of Nutrition in Sport
1. Carbohydrate, Protein, and Fat in Athletic Nutrition
Carbohydrates, protein, and fat are three macronutrients crucial in supporting athletic performance, including tennis. Carbohydrates are the primary energy source for the body and brain. At the same time, protein plays a role in building and repairing muscle tissue, and fat provides long-term energy and supports complex bodily functions. The importance of each of these macronutrients in supporting the performance of tennis athletes has been widely reviewed in the scientific literature. In tennis, carbohydrates are vital as energy is essential for maintaining athlete performance during long matches. A study published in research [6] stated that adequate carbohydrate intake can improve athlete endurance, slow the onset of fatigue, and support recovery after training or matches. Thus, tennis athletes must ensure the proper carbohydrate intake before, during, and after training or matches to maintain optimal performance. In addition to carbohydrates, protein also plays a vital role in supporting the performance of tennis athletes. Protein is required to repair and build muscle tissue damaged by training or matches and maintain optimal muscle strength and mass. A study found that adequate protein consumption, especially after training, can increase muscle protein synthesis and accelerate muscle recovery.
Therefore, tennis athletes must be mindful of their protein intake to support recovery and maximize muscle adaptation. Fat is also essential to a tennis athlete's diet, although it often receives a negative stigma associated with an increased risk of cardiovascular disease. However, fat is a necessary source of energy, especially for long-duration activities such as tennis matches that last up to several hours. A study [7] showed that fat can be an efficient energy source, especially in low to moderate-intensity activities. Therefore, tennis athletes must focus on healthy fat intake, especially from monounsaturated and polyunsaturated fat sources, to support their stamina and performance during matches. Overall, carbohydrates, protein, and fat are essential components in a tennis athlete's diet that support energy, muscle recovery, and optimal performance. Therefore, tennis athletes must pay close attention to their nutritional intake and ensure they get adequate macronutrients to reach their maximum potential.
2. Essential Vitamins and Minerals
Vitamins and minerals support optimal body function, especially in intense physical activities like tennis. Adequate nutrition can help maintain electrolyte balance, improve muscle recovery, and support the athlete's immune system. In sports, the right balance of vitamins and minerals can significantly affect an athlete's performance. Research has highlighted the importance of vitamins and minerals in sports. For example, a study by [8] states that vitamins and minerals play an essential role in forming enzymes involved in energy metabolism and supporting the immune system. This suggests that vitamins and minerals serve as cofactors in various metabolic processes and play a role in maintaining overall health.
In addition, studies have also shown a correlation between vitamin and mineral intake and athletic fitness. A study conducted by [9] found that athletes with adequate intake of vitamins and minerals tend to perform better and have faster recovery after training or competition [10]. It is confirmed that proper vitamins and minerals can support athletes' stamina and recovery, being essential in tennis, which requires high physical endurance. In addition to supporting physical aspects, vitamins and minerals also have a role in maintaining athletes' mental balance. A study by [11] found that specific vitamin and mineral deficiencies can contribute to decreased mood and concentration, affecting an athlete's overall performance [12]. Proper nutrition can help maintain athletes' mental balance, which is essential in competitive sports such as tennis.
However, it is essential to remember that an excess or deficiency of vitamins and minerals can also negatively impact athletes' health and performance. A study by [13] found that an excess or deficiency of specific vitamins and minerals can lead to health problems such as fatigue, reduced performance, and even injury in athletes. Therefore, it is essential to ensure a balanced and appropriate intake of nutrients according to individual needs. In addition, factors such as the environment and an individual's diet can also affect the nutritional status of athletes. A study conducted [14] concluded that factors such as diet, living habits, and environment can affect athletes' vitamin and mineral intake, making it essential to pay attention to these factors in planning athletes' diets [15]. Besides varying nutritional requirements, external factors must be considered when planning an athlete's diet.
Overall, vitamins and minerals play an essential role in supporting the performance and health of athletes, including tennis athletes. Adequate intake of these nutrients can help improve athletes' stamina, recovery, and mental balance. However, paying attention to individual needs and external factors in planning an athlete's diet to achieve optimal results is essential.
Previous Studies on Nutrition and Tennis
Previous research has revealed the significant impact of diet and supplementation on tennis athletes' performance. Through analyses of specific diets and supplement use, these studies highlight the relationship between nutrition and critical aspects of performance, such as stamina, strength, and recovery. With a focus on practical implications, the studies provide valuable insights into understanding how nutrition affects the overall performance of tennis athletes. Previous studies have examined the relationship between diet and tennis athlete performance. These studies considered general nutrient intakes and specialized diets, such as high-protein or low-carbohydrate diets. A study [16] concluded that a protein-rich diet can improve muscle recovery and strength, which is essential for tennis athletes who experience heavy loading in training and matches. A high-protein diet can also help maintain muscle mass and improve performance [17].
Aside from diet, supplementation has also been the focus of research to improve the performance of tennis athletes. Clinical studies suggest that creatine supplements, which are often used in power sports, may benefit tennis athletes by improving muscle strength and endurance. A study [18] mentioned that creatine can increase training volume and accelerate recovery after strenuous activity.
The importance of electrolytes and hydration has also been a significant research topic in tennis. Loss of electrolytes through sweat during a match can disrupt the ion balance in the body and affect the athlete's performance. In a study conducted [19], it was suggested that electrolyte drinks could help replace lost electrolytes and maintain hydration, thus improving the performance of tennis athletes during long matches. Protein supplements have also been the focus of significant research in the context of post-workout recovery. Athletes often use protein shakes to accelerate muscle recovery after intense exercise. A study by [20] found that consuming protein supplements after exercise can increase muscle protein synthesis and accelerate muscle recovery, thus allowing athletes to recover faster and return to training or matches better.
In addition to improving performance, nutrition also plays a role in reducing the risk of injury in tennis athletes. Diets rich in antioxidants, such as vitamins C and E, have been associated with reduced inflammation and cell damage, which may help prevent athlete injuries. A study by [21] showed that antioxidant supplements may reduce the risk of injury in athletes by reducing levels of inflammation and oxidative stress in the body. Nevertheless, it is also essential to consider the potential side effects of supplementation in athletes. Several studies have highlighted the risks associated with long-term supplement consumption, including digestive problems, kidney damage, and nutritional imbalances [22]. They concluded that a better understanding of the potential risks and benefits of supplementation is needed to inform better athlete nutrition decisions.
These studies clearly show that diet and supplementation play an essential role in improving tennis athletes' performance. Nevertheless, it is crucial to consider individual factors and the specific needs of the athlete when designing an effective and safe nutritional strategy.
Nutrition's Impact on Stamina, Strength, and Recovery
Nutrition plays a crucial role in supporting stamina, strength, and recovery in tennis athletes. Carbohydrates, proteins, fats, vitamins, and minerals have a significant impact on these aspects.
1. The Role of Carbohydrates in Stamina
Carbohydrates are the body's primary energy source, especially in intense physical activities like tennis. Studies have shown that adequate carbohydrate intake can increase athletes' stamina and extend the time before feeling fatigued. A study by [23] stated that appropriate carbohydrate intake in quantity and timing can improve athletes' endurance and performance, including tennis athletes who require substantial energy during long matches.
2. Effect of Protein on Strength and Recovery
Protein is necessary for building and repairing muscles after training or competition. Adequate protein consumption can also increase muscle strength and speed up recovery. According to a study Ihsan & Nasrulloh, (2023), protein supplementation after training can increase muscle protein synthesis and accelerate the recovery of damaged muscles, contributing to long-term increases in muscle strength
3. The Importance of Fat in Long-term Stamina
Although often considered a reserve fuel, fat also has a vital role in supporting stamina, especially in training or competitions that last for extended periods. Fat can provide gradual and long-lasting energy. A study Cao et al., (2021) showed that a high-fat diet can increase fat oxidation and enable energy maintenance at low to moderate intensities, which is essential for tennis athletes in matches that last long periods.
4. Vitamins and Minerals for Optimal Recovery
Vitamins and minerals are essential to the body's recovery after training or matches. Some vitamins and minerals, such as vitamins C, E, and zinc, have anti-inflammatory and antioxidant properties that can help reduce inflammation and muscle tissue damage. Research [26] showed that adequate intake of vitamins C and E could reduce the extent of muscle damage and optimize the recovery process in athletes after strenuous exercise.
5. Water is an Essential Nutrient for Stamina and Recovery
Water is an often overlooked nutrient, being vital for athletes' stamina and recovery. Dehydration can lead to decreased performance, increased risk of injury, and slow recovery. A study [27] confirmed that dehydration of just 2% of body weight could decrease athlete performance, emphasizing the importance of maintaining adequate hydration during training and competition.
6. Electrolyte Supplements to Support Stamina and Recovery
Electrolytes such as sodium, potassium, and magnesium are essential for maintaining body fluid balance, muscle contraction, and nerve function. In situations where athletes lose a lot of fluid through sweat, electrolyte supplements can help maintain electrolyte balance and prevent fatigue and muscle cramps. According to a study [28], electrolyte supplements can reduce the risk of fatigue, decreased performance, and injury in athletes exposed to hot and humid environmental conditions.
A deep understanding of the relationship between nutrition and critical aspects such as stamina, strength, and recovery is essential for tennis athletes. By paying attention to proper nutrition, tennis athletes can improve their performance and prolong endurance and sustainability in intense matches.
Gaps in the Literature
The study of nutrition's effect on tennis athletes' performance has become an increasing focus in the scientific literature. However, although many studies have been conducted in this field, some gaps still need to be addressed. One of these is the lack of recent research that specifically examines the influence of nutrition on tennis athlete performance. While many studies have been conducted in this field, some gaps still need to be addressed. One of these is the lack of recent research that specifically examines the influence of nutrition on tennis athlete performance.
According to research [14], although there is increasing interest in the role of nutrition in sports, specific research on nutrition and tennis tends to be underrepresented in the current scientific literature. This could lead to a lack of in-depth understanding of the relationship between proper nutrition consumption and the improved performance of tennis athletes.
Furthermore, another gap in the literature is the need for more research considering specific aspects of nutrition and tennis, such as the role of nutrition in injury recovery in tennis athletes. A study [29] showed that proper nutrition can speed up the recovery process and reduce the risk of injury in tennis athletes. However, research explicitly examining nutritional strategies for injury recovery in tennis is limited.
Due to the need for more recent research on nutrition and tennis, it is essential to expand research that integrates more advanced methodologies, such as prospective cohort studies and sophisticated experimental designs. A study [30] emphasized the importance of sophisticated methodological approaches in sports nutrition research to better understand the relationship between nutrition and athletic performance.
In addressing this gap in the literature, researchers need to direct their efforts towards deepening the understanding of the specific types of nutrients that have the most effect on tennis athletes' performance, as well as how the timing of nutrient intake can affect performance during training and matches. A study [16] showed that nutrient intake before, during, and after practice or matches can significantly impact tennis athletes' performance.
The objective of this systematic review is to analyze and synthesize existing scientific evidence regarding the effect of nutrition on the performance of tennis athletes. This review aims to explore various nutritional strategies and dietary patterns commonly applied by tennis players, as well as examine the relationship between specific nutrients or supplementation and key performance indicators such as endurance, strength, agility, and recovery. By evaluating the effectiveness of these nutrition interventions, this study seeks to provide a clearer understanding of how nutrition contributes to athletic performance in tennis. Additionally, this review intends to identify gaps in the current literature and offer recommendations for future research to support the development of more effective and evidence-based nutritional strategies for tennis athletes.
MATERIALS AND METHODS OF RESEARCH
The research method used in this article was a systematic review that followed the PRISMA guidelines. This approach allowed for the structured collation and analysis of previous studies relevant to nutritional influences on tennis athlete performance. PRISMA provides a clear and systematic framework for identifying, assessing, and synthesizing evidence from the available literature in a transparent and detailed manner. The PRISMA approach requires a pre-defined research protocol, with inclusion (Table 1) and exclusion criteria, and a comprehensive search strategy. In addition, the methodological quality assessment of studies included in this review will be conducted systematically according to PRISMA guidelines. Using a PRISMA-guided systematic review approach, this study aims to provide a comprehensive and reliable synthesis of the relationship between nutrition and tennis athletes' performance based on the literature evidence.
Criteria Description Inclusion Study Type: Research articles (observational studies, intervention studies, meta-analyses, systematic reviews). Research Subjects: Professional or amateur tennis athletes of varying ability levels. Type of Intervention: Studies that evaluate the effects of nutrition (e.g., diet, supplements) on the performance of tennis athletes. Language: Studies published in English or other languages, provided there is a translation available. Publication Time: Articles published within the timeframe (2013 to 2024). Exclusion Study Type: Non-research reviews (editorials, newspapers, and book reviews). Study Subjects: Studies conducted on subjects other than tennis athletes or subjects with certain medical conditions. Type of Intervention: Studies that do not focus on nutritional interventions or only evaluate other aspects of performance. Language: Articles written in a language other than English for which there is no translation. Time of Publication: Articles published within more than 11 yearsTable 1. Inclusion Criteria ↓
In the Selection Process stage, a literature search was conducted in reputable databases such as PubMed, Scopus, and Web of Science using related keywords such as "Tennis athlete nutrition," "Tennis supplementation and performance," and "athlete diet and physical fitness." The search was limited to articles published between 2013 to 2024 to ensure the inclusion of the most recent and relevant research. After the search, relevant articles were screened by title and abstract. Articles that fulfilled the inclusion criteria such as relevance to the research topic and appropriate research type were selected for full-text reading. Subsequently, articles that satisfy the requirements will be included in the analysis. During the selection process, article quality assessment criteria will also be applied to ensure methodological quality and relevance of findings to the research objectives. Using this approach, the most relevant and high-quality articles will be considered in the analysis, ensuring that the research has a solid and reliable foundation. The PRISMA flowchart illustrates the entire selection process, which increases transparency and makes it easier to understand the selection process (Fig.).
Figure. The PRISMA flowchart illustrates the entire selection process ↓
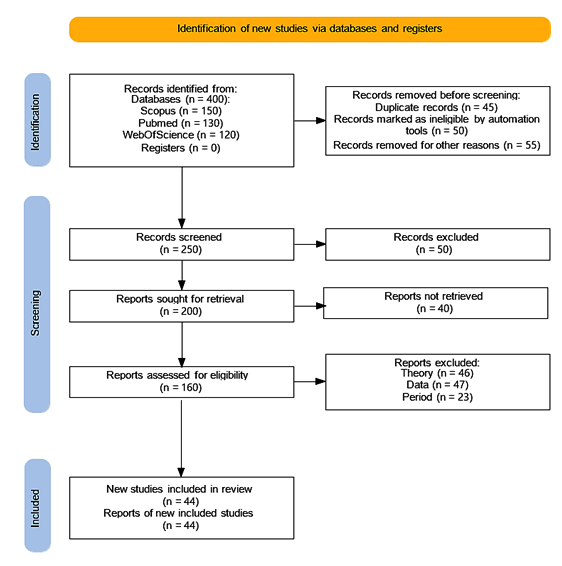
Data analysis in this study involved collecting and collating information from articles relevant to the topic. This process involved extracting data related to the nutrients studied, methods of measuring tennis athlete performance, and key findings from each article reviewed. The data were then analyzed to identify patterns or trends in the influence of nutrition on tennis athlete performance. The analysis approach may vary depending on the data collected, but generally includes grouping the data by relevant themes or variables and synthesizing the findings from the selected articles. Qualitative analysis methods may be used to understand the context and implications of the findings in depth.
In contrast, quantitative analyses, such as meta-analyses, may be used if sufficient data are available. Conclusions from these data analyses will help inform this systematic review's discussion and conclusions. PRISMA flowcharts will visualize the study selection and inclusion process, ensuring transparency and ease of understanding for the reader.
RESULTS AND DISCUSSION
In analyzing the findings regarding the influence of nutrition on the performance of tennis athletes, there are several essential aspects to consider (Table 2). First of all, carbohydrates, protein, and fat have a significant role in supporting the performance of tennis athletes. Carbohydrates are the primary source of energy for physical activity, which contributes to athletes' endurance and strength during matches. Research shows that adequate carbohydrate intake before and during matches can improve the performance of tennis athletes, especially in matches that require high intensity and last long [6]. On the other hand, protein is essential for maintaining and repairing muscles after training or matches. Adequate protein consumption can also help athletes build muscle mass and increase strength [36]. Fats, particularly healthy fats such as omega-3, have been shown to have anti-inflammatory effects that may help reduce the risk of injury and improve the cognitive function of tennis athletes [37].
Key Findings from Systematic Review Findings One of the supporting Journals of the Systematic Review Explanation Effects of Carbohydrate, Protein, and Fat [31, 32] Carbohydrate intake supports the stamina and energy that tennis athletes require during long, intensive matches. Protein has been shown to play an essential role in repairing and building muscle mass, which can help improve tennis athletes' physical strength and endurance. The right fats, especially polyunsaturated fats, can also support body function and nutrient absorption, essential for tennis athletes The Role of Vitamins and Minerals [1, 33, 34] Vitamins and minerals play a crucial role in supporting optimal body function, including strengthening the immune system, speeding up recovery, and maintaining electrolyte balance. Deficiencies in specific vitamins and minerals can negatively impact a tennis athlete's performance, that is why it is essential to ensure adequate intake of food or supplements Long-term and Short-term Impacts [14, 35] Proper nutritional intake can provide short-term benefits in improving performance immediately after consumption, as well as long-term benefits in sustaining and enhancing the performance of tennis athletes. Nutrients obtained from natural foods tend to provide better long-term benefits than nutritional supplements in maintaining athlete health and performanceTable 2. Findings in the Study ↓
In addition to macro-nutrients, vitamins, and minerals also have an essential role in improving the performance of tennis athletes. Vitamins such as vitamins C and E have antioxidant effects that can help in fighting oxidative damage that occurs during training or matches [21]. Minerals such as iron and calcium are also crucial for maintaining bone and muscle health and ensuring optimal muscle contraction during matches [38]. Proper nutritional intake can also help improve recovery and reduce the risk of injury in tennis athletes [39]. A consistent and balanced diet not only affects an athlete's performance immediately but can also have a long-term impact on an athlete's physical endurance from season to season [16].
Overall, the relationship between nutrition and tennis athlete performance is complex. Not only proper nutrition is necessary to improve current performance, but also to ensure the athlete's long-term health and reduce the risk of injury. Therefore, tennis athletes and coaching teams need to understand the importance of proper nutrition strategies and implement them in their training and competition. Thus, the effort required in planning and managing the diet of tennis athletes will not only help improve their current performance but will also provide long-term benefits to their health and career in the sport.
Importance of Nutrient Intake
Proper nutritional intake can contribute significantly to improving the stamina and strength of tennis athletes. Numerous studies have shown that sufficient carbohydrates can enhance physical endurance, which is a critical factor in long and intense tennis matches. For example, research [40] highlighted the importance of carbohydrates in improving long-term athletic performance by providing a sustainable source of energy for muscles during training and competition.
Proper nutrition also plays a vital role in supporting athletes' recovery process after training or competition. Protein, for example, is required to repair and rebuild muscles damaged during intense exercise or minor injuries during a match. According to research [41], adequate protein intake after training can increase muscle protein synthesis and accelerate muscle recovery associated with physical damage from exercise.
In addition to affecting physical aspects, nutritional intake can also have a positive impact on the mental and cognitive performance of tennis athletes. Specific vitamins and minerals, such as B-complex vitamins and magnesium, have been shown to play an essential role in neural function and mental concentration. A study [42] found that vitamin B complex supplements can improve cognitive performance and mood stability, which can benefit tennis athletes in maintaining focus and concentration during long, stressful matches.
While nutritional supplements are often an easy option, it's important to remember that natural sources of nutrients, such as whole foods, are also crucial for athletes' health and performance. A study by [43] highlighted that natural foods often provide nutrients in a more complete form and are easily absorbed by the body compared to supplements, which can have different side effects and tolerance in individuals.
By paying attention to proper nutrition intake, tennis athletes can maximize their physical and mental potential, improving endurance, strength, and focus, all of which are important in achieving peak performance in this demanding sport.
The results of this systematic review show that nutrition plays a crucial role in improving athlete performance. Interpretation of the findings suggests that various aspects of nutrition, such as carbohydrates, proteins, fats, vitamins, and minerals, have a significant impact on tennis athletes' stamina, strength, and recovery. For example, carbohydrates play an essential role in providing the energy required to endure intense training sessions and long matches. Proteins are needed to repair and build muscle after a workout or match. At the same time, fats provide lasting energy and aid in the absorption of specific vitamins that are essential for optimal body function.
The implications of these findings are clear. Tennis coaches, nutritionists, and athletes can use this information to design appropriate nutritional strategies to improve athlete performance. Practical recommendations include paying attention to the composition of meals before and after training sessions or matches, ensuring athletes have adequate intake of each type of nutrient required to maintain optimal health and performance. It is also essential to consider the individual needs of each athlete, as the body's response to nutrients can vary significantly between individuals.
However, while these findings provide valuable insights, some limitations need to be recognized. The systematic review method has the potential for bias in article selection and data interpretation. In addition, there are shortcomings in the literature that may affect the generalisability of the findings, such as the lack of studies examining the direct influence of nutrition on tennis athletes. This suggests the need for further research to understand more deeply the interaction between nutrition and performance in tennis athletes.
In the context of future research, it is essential to consider better research designs that allow the identification of causality between nutrient intake and the performance of tennis athletes. Longitudinal studies with larger samples may provide a more comprehensive insight into the impact of nutrition on tennis athletes' performance over time. In addition, there is a need for research that takes into account other factors that may influence the relationship between nutrition and performance, such as psychological and environmental factors.
In conclusion, while these findings provide strong evidence of the influence of nutrition on the performance of tennis athletes, further research is needed to understand in greater depth the complexity of this relationship. However, by paying attention to proper nutrition, tennis athletes can improve their performance and reach their maximum potential in their sport.
CONCLUSIONS
Acknowledgments.
The authors would like to thank all the team of authors included in this article who have helped in writing and analyzing this systematic review article very well.
Contributors:
Sayuty Yogi – conceptualization, validation, resources, funding acquisition, investigation, data curation, formal analysis;
Sabillah Muhamad Ichsan – software, writing – original draft, methodology, formal analysis, Investigation;
Hidayat Rezha Arzhan – data curation, visualization, supervision, project administration;
Sholichah Ima Fitri – writing – review & editing, software.
Funding. This research received no external funding.
Conflict of interests. The authors declare no conflict of interest.
REFERENCES
 UK
UK  EN
EN 