
 UK
UK  EN
EN 

I.S. Borysova *
![]() D.O. Safonov
D.O. Safonov
![]()
Key words: disability, acute cerebral stroke, functional impairment, adult population, labor force
Ключові слова: інвалідність, гострий мозковий інсульт, порушення життєдіяльності, доросле населення, працездатне населення
Abstract
Acute cerebral stroke is a disease that ranks among the leading causes of today's “non-infectious” epidemic, becoming a significant economic burden for global economies. The aim of the study was to investigate the dynamics of disability rates due to acute cerebral stroke and their features among the adult and working-age population in Ukraine under conditions of martial law. This work is fragment of the DSMU research project “Improvement of scientific and methodological approaches to determining the criteria for identifying signs of permanent disability, optimization of rehabilitation programs for patients and persons with disabilities”, No. 0124U005028, 2025-2028. Medical and social cases and referrals for medical and social examination (Form 088/o) of patients who were diagnosed with disability for the first time during the period of 2014-2024 were analyzed in accordance with ICD-10 codes: stroke (I 60 I 64), hemorrhagic stroke (I 60, I 61, I 62), ischemic stroke (I 63, I 64), and consequences of stroke (I 69). Statistical processing was performed using parametric and nonparametric statistical methods implemented in the STATISTICA 6.1 software package (StatSoftInc., serial number AGAR909E415822FA).The results of the study conducted over the last decade from 2013 to 2024 in Ukraine determined the dynamics of primary disability rates due to acute cerebral stroke. Among the adult and working-age population during 2011-2019, a stable dynamic of the indicator was found, which averaged 1.67 per 10,000 people, with a minimum level in 2020 – 1.3 and 1.7 per 10,000 people, respectively. The conclusions of the study are the identified characteristics of primary disability rates due to acute cerebral stroke ubder conditions of martial law. In 2022-2024, an increase in this indicator among both the adult and working-age population was identified, being approximately twice as compared to pre-war indicators.
Реферат
Інвалідність унаслідок гострих мозкових інсультів в Україні за період 2014-2024 років та особливості динаміки в умовах воєнного стану. Борисова І.С., Сафонов Д.О. Гострий мозковий інсульт є захворюванням, що займає основні позиції серед причин неінфекційної епідемії сьогодення, стаючи значним економічним тягарем для світових економік. Метою роботи було дослідити динаміку показників інвалідності серед дорослого та працездатного населення внаслідок гострого мозкового інсульту в Україні та їх особливості в умовах воєнного стану. Робота є фрагментом НДР ДДМУ «Удосконалення науково-методичних підходів до визначення критеріїв визначення ознак стійкої непрацездатності, оптимізації програм реабілітації хворих та осіб з інвалідністю», № 0124U005028, 2025-2028 рр. Проаналізовано медико-соціальні справи та направлення на медико-соціальну експертизу (форма 088/о) пацієнтів, яким було встановлено інвалідність уперше за період 2011-2024 рр. відповідно до кодів МКБ Х: інсульт (I 60 I 64), геморагічний інсульт (I 60, I 61, I 62), ішемічний інсульт (I 63, I 64), наслідки інсульту (I 69). Статистична обробка проводилась методами параметричної та непараметричної статистики, реалізованими в пакетах програмних продуктів STATISTICA 6.1 (StatSoftInc., серійний № AGAR909E415822FA). Результатами проведеного дослідження за період останнього десятиріччя з 2011 до 2024 року в Україні визначено динаміку показників первинної інвалідності внаслідок гострого мозкового інсульту. Серед дорослого і працездатного населення впродовж 2011-2019 рр. виявлено стабільну динаміку показника, який становив у середньому 1,67 на 10 тис. нас. з мінімальним рівнем у 2020 р – 1,3 та 1,7 на 10 тис. нас. відповідно. Висновками дослідження є визначені особливості показників первинної інвалідності внаслідок гострого мозкового інсульту в період воєнного стану. У 2022-2024 роках визначено підвищення цього показника як серед дорослого, так і працездатного населення приблизно у 2 рази порівняно з довоєнними показниками.
Acute cerebral stroke (ACS) is a disease that occupies a leading position among the causes of the “non-infectious” epidemic of today, becoming a significant economic burden for world economies.
In 2017, 1.5 million people in 32 European countries suffered from ACS, while 0.4 million of them died. At the same time, direct costs for care for ACS amounted to 27 billion euro, which amounted to 1.7% of healthcare expenditures in Europe as a whole [1]. In the same year, according to the Global Burden of Disease study, 24.1 million of new cases of ACS were registered worldwide [2]. And already in 2019 this figure reached 101 million (93.2-111) of common ACS and 6.55 million (6.00-7.02) of deaths from stroke, ranking second among the leading causes of death globally, accounting for 11.6% [10.8-12.2] of the total number of deaths recorded in 2019. According to the analysis, the dynamics is disappointing: from 1990 to 2019, the absolute number of strokes increased by 70.0% (67.0-73.0) [3]. At the same time, it is predicted that in the coming decades, the number of cases of ACS will increase by 34%, which will lead to a 27% increase in costs, amounting to 1.7% of total healthcare costs [1]. It is known that direct medical costs per patient with ACS in the first year are $59,900 in the USA, $52,725 in Sweden, and $41,950 in Spain [4].
According to estimates by the National Health Service (NHS) in Ukraine in 2021, 118 thousand cases of ACS were diagnosed, and already in 2024 the number of hospitalizations for this reason reached 137.6 thousand cases, which is by 16% higher. Diagnosis and treatment of ACS in Ukraine are completely free of charge, as they are a priority service in the Medical Guarantees Program. Currently, there are 229 healthcare institutions (HCIs) in the country that provide care for ACS. For the treatment of one patient with ACS, the HCI receives 131,472 hryvnias from the National Health Service of Ukraine (NHSU) for the provision of care with the use of endovascular interventions; 62,565 hryvnias for care with the use of thrombolytic therapy; 14,952 hryvnias for care without endovascular interventions or thrombolytic therapy. In 2023 alone, under the “Medical Care for ACS” package, Ukrainian HCIs received reimbursement of over 1.7 billion hryvnias for the services provided [5]. Unfortunately, the mortality rate from ACS in Ukraine remains 2-3 times higher than in the EU: in 2024, the hospital mortality rate was 16.62%, and the 30-day mortality rate was 21.85%. In September 2025, the fourth UN meeting on non-communicable diseases noted that the European target of reducing mortality by 1/3 by 2030 had not yet been achieved, and that prevention was the key to progress [5].
It is also important to note that the consequences of ACS among surviving patients are becoming one of the leading causes of disability in the world, despite modern advances in methods [6]. In both the United States and European countries, ACS remains the leading neurological disease in terms of the number of DALYs (Disability-Adjusted Life Years) – an indicator of "life years adjusted for disability", which measures the total "burden" of disease, disability and premature death. The indicator is equal to the time of healthy life lost due to premature death or disability [7]. Thus, the financial burden of ACS on society is enormous, taking into account rehabilitation services, costs of homes for people with additional supervision and assistance with self-care, reimbursement of drug costs by insurance, informal care from the state, volunteers or relatives and potential loss of earnings. Thus, the DALY indicator in 2017 amounted to 15.7 million disability-adjusted life years [8]. And in 2019, the global economy lost 143 million (133-153) years of life due to ACS. The consequences of ACS have become the third leading cause of disability in the world, with an increase in DALYs by 32.0% (22.0-42.0) and a decrease in life expectancy by 36.0% (31.0-42.0) compared to studies done in 2017 [3]. Indirect costs of ACS in Europe include social security for people who have suffered ACS, which is estimated at €5 billion. The annual cost of caring for people with GMI in 2019 was €59 per EU citizen on average, ranging from €11 in Bulgaria to €140 in Finland. Productivity losses cost the European economy €12 billion, and were divided equally between causes of premature death and lost working hours. In total, €1.3 billion in informal care hours were provided to people who had suffered a stroke, costing Europe another €16 billion. [1]. The highest costs per patient after a stroke over a lifetime were recorded in Australia, which amounted to $232,000 [9].
In the USA, indirect costs exceed 60% of total costs for ACS and amount to $103.5 billion as of the beginning of 2020, with a loss of productivity due to disability, being $38.1 billion [10]. At the same time, according to the calculations of the American Heart Association, the average cost of treatment for a person who has suffered ACS may exceed $100 thousand. [11]. Linear interpolation shows that if current trends continue, by 2050, there will be up to 200 million people with the past stroke worldwide annually, who will need rehabilitation and social assistance, which will inevitably lead to a 27% increase in medical and social assistance costs, which will approach 1.7% of total global health care costs [1].
It is also important to emphasize that in Ukraine among people with past ACS about 35% are those of working age. According to official data, from 20 to 40% of people who have survived ACS cease to be independent and are completely dependent on outside help, another 12.5% fall into the category of primary disability. And only 10% return to the state they had before the onset of the disease. Such annual losses cannot but affect the state economy. According to some scientists, the total losses of the Ukrainian economy associated with the consequences of ACS can reach about 100 billion UAH per year [12]. The Framingham study showed that after past ACS, signs of disability were formed in 22-40% of patients after 6 months [13], and after 1 year - in almost 50% [14]. The share of people with disabilities due to ACS in China in 2020 was 63.8%; including the share of mild, moderate, severe and complete disability – 30.1%, 18.0%, 10.7% and 5.0% respectively [15]. According to the Korean National Survey for the period of 2007-2018 (KNHANES), it is known that 38.0% of those who survived ACS became disabled [16].
According to previous studies, in Ukraine in 2009, among people with past ACS of all forms, 32.7% died, and 7.8% received one or another degree of disability [17]. It is known that among the main groups of disabling diseases, cerebrovascular diseases (the main contribution among which is the consequences of ACS) rank forth among the main causes of disability by the cause of “general disease” (after neoplasms, injuries and diseases of the musculoskeletal system and connective tissue) both among the adult and among the able-bodied population [17].
The aim of the study was to investigate the dynamics of disability rates due to acute cerebral stroke and their features among the adult and working-age population in Ukraine under conditions of martial law.
MATERIALS AND METHODS OF RESEARCH
The work is a fragment of the research work (R&D) of the Department of Medical and Social Expertise and Rehabilitation of the Dnipro State Medical University (DSMU) "Improvement of scientific and methodological approaches to determining the criteria for limiting vital activity due to the consequences of injuries and diseases (in the system of medical and social expertise)", No. 0121U100080, 2021-2024 and "Improvement of scientific and methodological approaches to determining the criteria for determining signs of persistent disability, optimizing rehabilitation programs for patients and persons with disabilities", No. 0124U005028, 2025-2028. By its type the research consisted of two stages. In the course of the research, primary disability indicators in Ukraine according to state statistical materials and data of scientific literature during 2010-2019 were studied [17, 18]. The next stage of the work was carried out at the clinical base of the state institution “Ukrainian State Scientific Research Institute of Medical and Social Problems of Disability of the Ministry of Health of Ukraine” according to the reports of regional centers of medical and social expertise (MSE) during 2020-2024. The MSE commissions [19] were asked to submit aggregate statistical information according to the ICD codes: cerebrovascular pathology: stroke (I 60 I 64), hemorrhagic stroke (I 60, I 61, I 62), ischemic stroke (I 63, I 64), consequences of stroke (I 69) and transient ischemic attacks (G 45). We analyzed the medical and social cases and referrals for medical and social expertise (Form 088/o) of 29,024 patients who were examined by specialized cardio-neurological commissions and formed the study group, quantization by years: 2021 – 4,619 people; 2022 – 7,219 people; 2023 – 9,431 people; 2024 – 7,779 people. The disability criteria were considered to be persistent functional impairments, associated limitations in life activity criteria and the need for state assistance, in accordance with the regulatory documents in force at the time of the study [20].
The research calculated intensive indicators of the prevalence of primary disability due to ASC among adults and able-bodied people (per 10,000 population) and specific gravity (in %), their dynamics over the period of the 2011-2024 was studied [21]. In connection with the declaration of martial law in Ukraine on February 22, 2022, the State Statistics Service put on pause the publication of data on the demographic situation in Ukraine, which does not allow the calculation of real intensive indicators for 2022, 2023 and 2024. In this regard, the calculation of intensive indicators was carried out based on the latest state statistical data by regions of Ukraine as of January 1, 2022 [22].
The processing of the obtained research results using biostatistical methods was carried out using the STATISTICA v.6.1 software product (StatsoftInc., USA), license number AGAR909E415822FA. In particular, an analysis of the 10-year dynamics of disability indicators was carried out with the calculation of average growth rates (Δ) according to the formula:
where
X – is the studied indicator for a specific year of statistical observation;
10 – is the number of years of observation.
The study was conducted in compliance with the basic norms of bioethics and the requirements of the Helsinki Declaration on Human Rights and Biomedicine (1977) and relevant laws of Ukraine and was permitted by the Commission on Biomedical Ethics of the DSMU (Protocol No. 32 dated November 11, 2025).
RESULTS AND DISCUSSION
Figures 1 and 2 present the determined intensive indicators of primary disability due to ACS in Ukraine, calculated per 10 thousand population for the period of 2011-2024 among the adult and working-age population, respectively. The prevalence rate of primary disability among the adult population of Ukraine due to the consequences of ACS was: 1.9 per 10 thousand population in 2011; 1.6 – in 2012; 1.8 – in 2013; 1.7 – in 2014; 1.6 – in 2015; 1.5 – in 2016; 1.6 – in 2017; 1.8 – in 2018; 1.6 – in 2019; 1.3 – in 2020; 1.5 – in 2021; 2.1 – in 2022; 3.1 – in 2023, and 3.1 – in 2024.
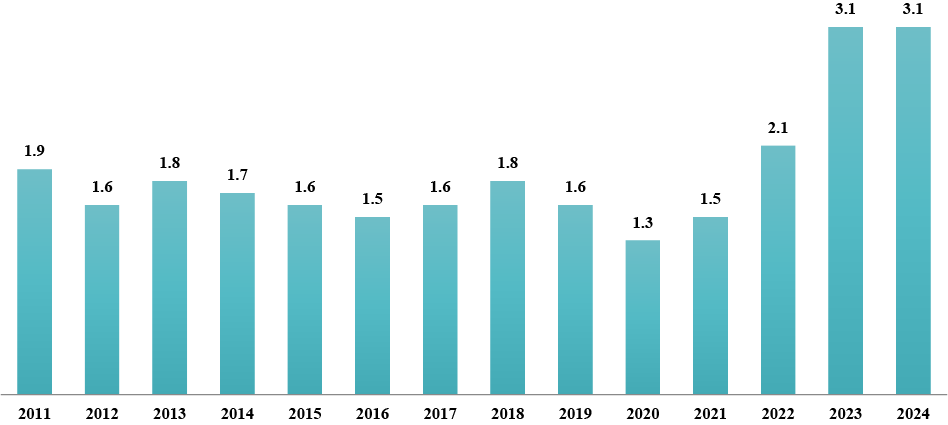
Thus, a stable dynamics of the prevalence rate of primary disability among the adult population during 2011-2019 was revealed – from 1.9 in 2011 to 1.6 in 2019. During this period, the rate averaged 1.67 per 10 thousand people. It is important to note that well-known Ukrainian epidemiological studies on the “consequences of stroke”, which were the cause of primary disability over the period of 2002-2012 in Ukraine also determined a certain stable dynamics and were, respectively: 10.3; 10.3; 9.4; 10.7; 12.3; 10.6; 9.3; 9.0-10.1; 9.7 people per 100 thousand adults[18]. Other researchers also determined the absence of significant changes in the rate of primary disability due to ACS among the adult population in 2008-2010, which was 10.6-9.3-9.9 cases per 100 thousand people [17]. In our study, the minimum prevalence rate of primary disability among the adult population was determined in 2020, which was 1.3 per 10 thousand people, with a slight increase in 2021 to 1.5 per 10 thousand people. A significant increase in the indicator was found during the martial law period, when the indicator grew from 2.1 in 2022 to 3.1 in 2023-2024. The increase in the indicator during the war years grew by 1.6 times (+51.6%) compared to the stable period. The average annual growth rate (Δ) for the studied period was 0.277 or 27.7% per year.
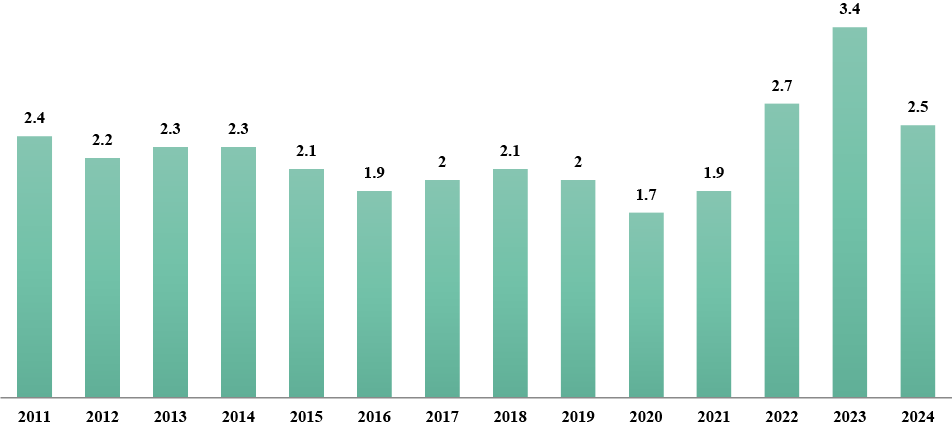
The prevalence rate of primary disability of the working-age population due to the consequences of ACS in Ukraine in 2011 was 2.4 per 10,000 population, in 2012 – 2.2; in 2013 – 2.3; in 2014 – 2.3; in 2015 – 2.1; in 2016 – 1.9; in 2017 – 2.0; in 2018 – 2.1; in 2019 – 2.0; in 2020 – 1.7; in 2021 – 1.9; in 2022 – 2.7; in 2023 – 3.4 and in 2024 – 2.5.
Among the working-age population, the results of the study revealed a stable dynamics of the prevalence rate of primary disability during 2011-2019 – from 2.4 in 2011 to 2.0 in 2017-2019. During this period, the rate averaged 2.4 per 10 thousand people. The minimum rate of primary disability among the working-age population was determined in 2020, being 1.7 per 10 thousand people, with an insignificant increase to 1.9 per 10 thousand people in 2021. During the period of martial law in 2022-2024, a significant increase in this rate among the working-age population was detected, which rose to 3.4 per 10 thousand people in 2023. At the same time, the increase in the indicator during the war years was 1.7 times (+50%) as compared to the stable period. The average annual growth rate (Δ) for the studied period was 0.094 or 9.4%.
In the process of discussing the results obtained, it is important to emphasize the reasons for the consistent decrease in primary disability rates up to 2020, both among adults and the able-bodied population, due to the fact that in these years the state introduced contracting of health care institutions (HCIs) through the NHSU with clear requirements for the provision of primary care for ACS and a list of mandatory diagnostic and treatment procedures. In 2020 alone, the NHSU contracted 192 HCIs to provide care to patients with ACS, reimbursing over 965 million UAH. At the same time, in Ukraine, 31,151 patients received primary care for ACS [23]. In the case of therapeutic endovascular interventions, the NHSU tariff for 1 person is over 97 thousand hryvnias, and the cost of ACS treatment using thrombolytic therapy is 54 thousand hryvnias [24]. In the same year, the Order of the Ministry of Health on the organization of medical care for patients with suspected ACS in the emergency medical care system was updated [25]. A significant increase in the rate of primary disability due to ACS during the period of martial law, both among the adult and able-bodied population of Ukraine, despite the adoption of new standards for providing care for ischemic and hemorrhagic types of ACS is noteworthy [26]. The increase in disability rates due to ACS in 2021 can be explained by the accumulation of disabling consequences of strokes associated with COVID-19. Neurological complications of COVID-19 are known to occur in more than a third of patients [27]. In patients with severe SARS-CoV-2 infection requiring intensive care unit treatment, the prevalence of neurological complications was as high as 84% [28]. The incidence of ACS in one of the first studies of neurological complications of COVID-19 in Wuhan was 2.34%. A large-scale meta-analysis including 24 cohort studies and more than 108 patients with COVID-19 found the incidence of ACS to range from 0.4 to 8.1% [29], making it the most common neurological complication among hospitalized patients with COVID-19 [30].
The reasons for the further increase in disability rates during the martial law period, which undoubtedly affected both the adult and working-age population of Ukraine, are special. Thus, it is known that the impact of armed conflicts significantly affects the increase in the prevalence of CVD with a chronic and acute course [31]. As a rule, this occurs due to the increase in the prevalence of risk factors associated with martial law, in particular, this has been confirmed in national studies of recent years: acute events on the background of CVD due to chronic or acute stress increased by 4.3 times and by 2 times due to excessive alcohol consumption [32]. Ukrainian researchers record an increase in the number of ACS by 22% against the background of an increase in the total number of hospitalizations in some front-line areas up to 60% [33]. Thus, according to the National Health Service, the regions where the largest number of patients with ACS were treated in 2023 are: Dnipropetrovsk (8,176 people), Kharkiv (6,443 people), Kyiv (5,993 people) and Lviv (5,184 people) regions and the city of Kyiv (7,889 people). It is these features of the course of ACS in modern conditions that have become the reasons for the increase in the rate of primary disability among Ukrainians of working age.
The features of understanding “disability” as a social phenomenon are: persons with disabilities in any state have the right to certain social measures of protection and assistance. As for the disability rate due to ACS among the adult population, it should be understood that under martial law, this rate increased due to the so-called “hidden disability”. In Ukraine, it is legally established that a person is not entitled to receive several social material benefits at the same time. Thus, some actual persons with disabilities due to ACS who reached retirement age did not apply for disability status before the war. At the same time, under martial law, these persons were forced to apply for this status in connection with other social benefits related to the specifics of this period.
CONCLUSIONS
1. The results of the study conducted in Ukraine for the period from 2011 to 2024 determined the dynamics of primary disability indicators due to acute cerebral stroke. Among the adult and able-bodied population during 2011-2019, a stable dynamics of this indicator was found, being an average of 1.67 per 10 thousand people with a minimum level in 2020 – 1.3 and 1.7 per 10 thousand people, respectively.
2. The study identified certain features of primary disability indicators due to acute cerebral stroke under the conditions of martial law. In 2022-2024, an increase in this indicator was established among both the adult and able-bodied population by approximately 2 times compared to the pre-war period. This may be explained by a number of factors, including: increased prevalence of risk factors, stress associated with martial law, and the phenomenon of “hidden disability.”
Contributors:
Borysova I.S. – conceptualization, methodology, formal analysis, visualization, writing – review & editing, project administration;
Safonov D.O. – investigation, resources, visualization, writing – original draft.
Funding. The article is a fragment of the scientific and research work of DSMU "Improvement of scientific and methodological approaches to determining the criteria for limiting vital activity due to the consequences of injuries and diseases (in the system of medical and social expertise)", No. 0121U100080, 2021-2024 and "Improvement of scientific and methodological approaches to determining the criteria for identifying signs of persistent disability, optimization of rehabilitation programs for patients and persons with disabilities" No. 0124U005028, 2025-2028.
Conflict of interests. The authors declare no conflict of interest.
REFERENCES
1. Luengo-Fernandez R, Violato M, Candio P, Leal J. Economic burden of stroke across Europe: A population-based cost analysis. Eur Stroke J. 2020 Mar;5(1):17-25. doi: https://doi.org/10.1177/2396987319883160
2. GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019 May;18(5):439-58. doi: https://doi.org/10.1016/S1474-4422(19)30034-1
3. GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021 Oct;20(10):795-820. doi: https://doi.org/10.1016/S1474-4422(21)00252-0
4. Strilciuc S, Grad DA, Radu C, Chira D, Stan A, Ungureanu M, et al. The economic burden of stroke: a systematic review of cost of illness studies. J Med Life. 2021 Sep-Oct;14(5):606-19. doi: https://doi.org/10.25122/jml-2021-0361
5. Shepelya V. [How much does the National Health Insurance Fund pay to medical institutions for the treatment of each patient with a stroke?]. [Internet]. 2024 [cited 2025 Aug 25]. Ukrainian. Available from: https://medicine.rayon.in.ua/news/670492-skilki-platit-nszu-medzakladam-za-likuvannya-kozhnogo-patsienta-z-insultom
6. Benjam EJ, Munter P, Alonso A, Bittencourt Refer MS, Calloway CW, Carson AP, et al. Heart sickness A stoke information-2019 update: A report from the yank heart affiliation flow. Circulation. 2019;139(10):e56-C528. doi: https://doi.org/10.1161/CIR.00000000000000659
7. GBD 2017 US Neurological Disorders Collaborators. Burden of Neurological Disorders Across the US From 1990-2017: A Global Burden of Disease Study. JAMA Neurol. 2021 Feb 1;78(2):165-76. doi: https://doi.org/10.1001/jamaneurol.2020.4152
8. Krishnamurthi RV, Ikeda T, Feigin VL. Global, Regional and Country-Specific Burden of Ischaemic Stroke, Intracerebral Haemorrhage and Subarachnoid Haemorrhage: A Systematic Analysis of the Global Burden of Disease Study 2017. Neuroepidemiology. 2020;54(2):171-9. doi: https://doi.org/10.1159/000506396
9. Strilciuc S, Grad DA, Radu C, Chira D, Stan A, Ungureanu M, et al. The economic burden of stroke: a systematic review of cost of illness studies. J Med Life. 2021 Sep-Oct;14(5):606-19. doi: https://doi.org/10.25122/jml-2021-0361
10. Girotra T, Lekoubou A, Bishu KG, Ovbiagele B. A contemporary and comprehensive analysis of the costs of stroke in the United States. J Neurol Sci. 2020 Mar 15;410:116643. doi: https://doi.org/10.1016/j.jns.2019.116643
11. The True Cost of a Stroke in the US [Internet]. Resolve. 2023 Oct 31 [cited 2025 Sep 15]. Available from: https://www.resolvemedicalbills.com/blog/the-true-cost-of-a-stroke-in-the-us
12. [Stroke statistics in Ukraine. Life-House Stroke Rehabilitation Center]. Health of Ukraine in the 21st century [Internet]. 2025 [cited 2025 Aug 10];7(593). Ukrainian. Available from:
https://life-house.center/statystyka-insultiv-v-ukrain/
13. Kelly-Hayes M, Beiser A, Kase CS, Scaramucci A, D'Agostino RB, Wolf PA. The influence of gender and age on disability following ischemic stroke: the Framingham study. J Stroke Cerebrovasc Dis. 2003 May-Jun;12(3):119-26. doi: https://doi.org/10.1016/S1052-3057(03)00042-9
14. Jönsson AC, Delavaran H, Iwarsson S, Ståhl A, Norrving B, Lindgren A. Functional status and patient-reported outcome 10 years after stroke: the Lund Stroke Register. Stroke. 2014 Jun;45(6):1784-90. doi: https://doi.org/10.1161/STROKEAHA.114.005164
15. Lv Y, Sun Q, Li J, Zhang W, He Y, Zhou Y. Disability Status and Its Influencing Factors Among Stroke Patients in Northeast China: A 3-Year Follow-Up Study. Neuropsychiatr Dis Treat. 2021;17:2567-73. doi: https://doi.org/10.2147/NDT.S320785
16. Ju YW, Lee JS, Choi YA, Kim YH. Causes and Trends of Disabilities in Community-Dwelling Stroke Survivors: A Population-Based Study. Brain Neurorehabil. 2022;15(1):e5. doi: https://doi.org/10.12786/bn.2022.15.e5
17. Khobzey NK, Mishchenko TS, Golik A, Gondulenko NA. [Features of Epidemiology of disability in diseases of the nervous system in Ukraine]. Mezhdunarodnyi nevrologicheskii zhurnal. [Internet]. 2011 [cited 2025 Aug 10];5(43):15-9. Russian. Available from: https://www.mif-ua.com/archive/article/21505
18. Golik VA, Gondulenko NA, Moroz YeN, Boguslavskii DD, Pogorelova VA. [Peculiarities of the epidemiology of disability in diseases of the nervous system in Ukraine: clinical and expert comparisons (10-year Ukrainian experience)]. Ukrainskyi visnyk medyko-sotsialnoi ekspertyzy. [Internet]. 2013 [cited 2025 Nov 10];7(1):33-41. Russian. Available from: http://irbis-nbuv.gov.ua/cgi-bin/irbis_nbuv/cgiirbis_64.exe?C21COM=2&I21DBN=UJRN&P21DBN=UJRN&IMAGE_FILE_DOWNLOAD=1&Image_file_name=PDF/ujmse_2013_1_7.pdf
19. [Issues of medical and social expertise. Resolution of the Cabinet of Ministers of Ukraine No. 1317 of 3.12.2009 (as amended in accordance with Resolutions of the Cabinet of Ministers No. 752 of 18.08.2010, No. 762 of 20.07.2011; No. 485 of 31.05.2012; No. 482 of 26.06.2015; No. 874 of 21.10.2015; No. 569 of 31.08.2016)]. [Internet]. 2016 [cited 2025 May 02]. Ukrainian. Available from: http://zakon3.rada.gov.ua/laws/show/1317-2009-%D0%BF
20. [Some issues of introducing assessment of daily functioning of a person. Resolution of the Cabinet of Ministers of Ukraine No. 1338 of 2024 Nov 15 [Internet]. 2024 [cited 2025 Jul 21]. Ukrainian. Available from: https://zakon.rada.gov.ua/laws/show/1338-2024-%D0%BF#Text
21. Hruzieva TS, Lekhan VM, Ohniev VA, et al. [Public Health: textbook]. [Internet]. Vinnytsia: New book; 2023 [cited 2025 Jul 21]. Ukrainian. Available from: http://ir.librarynmu.com/bitstream/123456789/11903/1/Громадське%20здоров%27я%202023.pdf
22. [Population of Ukraine – 2021: statistical collection]. [Internet]. Kyiv: State statistics service of Ukraine; 2022 [cited 2026 Nov 10]. Ukrainian. Available from: https://www.ukrstat.gov.ua/druk/publicat/kat_u/2022/zb/10/zb_nasel%20_2021.pdf
23. [The National Health Insurance Fund of Ukraine paid over UAH 965 million to medical institutions for providing assistance to patients with heart attacks and strokes]. LB.ua [Internet]. 2020 Sep 22 [cited 2025 Jul 09]. Ukrainian. Available from: https://lb.ua/society/2020/09/22/466514_nszu_viplatila_medzakladam_ponad_965.html
24. [The NHSU pays for the treatment of each stroke patient: assistance can be obtained in 238 hospitals across the country]. Government portal [Internet]. 2021 Oct 28 [cited 2025 Oct 13]. Ukrainian. Available from: https://www.kmu.gov.ua/news/za-likuvannya-kozhnogo-paciyenta-z-insultom-platit-nszu-otrimati-dopomogu-mozhna-u-238-likarnyah-po-vsij-krayini
25. [On approval of the Procedure for organizing the provision of medical care to patients with suspected acute cerebral stroke in the emergency medical care system. Order of the Ministry of Health of Ukraine No. 2203 dated 2020 Sept 25]. [Internet]. 2020 [cited 2025 Oct 09]. Ukrainian. Available from: https://zakon.rada.gov.ua/laws/show/z1120-20#Text
26. [On approval of the Standard of medical care «Ischemic Stroke». Order of the Ministry of Health of Ukraine dated 2024 Jun 20, No. 1070]. [Internet]. 2024 [cited 2025 Oct 09]. Ukrainian. Available from: https://moz.gov.ua/uk/decrees/nakaz-moz-ukrayini-vid-20-06-2024-1070-pro-zatverdzhennya-standartu-medichnoyi-dopomogi-ishemichnij-insult
27. Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020 Jun 1;77(6):683-90. doi: https://doi.org/10.1001/jamaneurol.2020.1127
28. Helms J, Kremer S, Merdji H, Clere-Jehl R, Schenck M, Kummerlen C, et al. Neurologic Features in Severe SARS-CoV-2 Infection. N Engl J Med. 2020 Jun 4;382(23):2268-70. doi: https://doi.org/10.1056/NEJMc2008597
29. Nannoni S, de Groot R, Bell S, Markus HS. Stroke in COVID-19: A systematic review and meta-analysis. Int J Stroke. 2021 Feb;16(2):137-49. doi: https://doi.org/10.1177/1747493020972922
30. Jawad M, Vamos EP, Najim M, Roberts B, Millett C. Impact of armed conflict on cardiovascular disease risk: a systematic review. Heart. 2019 Sep;105(18):1388-94. doi: https://doi.org/10.1136/heartjnl-2018-314459
31. Jawad M, Vamos EP, Najim M, Roberts B, Millett C. Impact of armed conflict on cardiovascular disease risk: a systematic review. Heart. 2019 Sep;105(18):1388-94. doi: https://doi.org/10.1136/heartjnl-2018-314459
32. Okunieva S-MS, Prokopiv MM. [The impact of military events on risk factors for cerebral stroke among residents of Kyiv]. Ukrainian Medical Journal. 2025;1:113-5. Ukr. doi: https://doi.org/10.32471/umj.1680-3051.260598
33. Shkoruta DP, Senkiv V, Vovchuk V, Popadynets O, Kotyk T. Impact of war on stroke incidence in Ivano-Frankivsk, Ukraine. Sci Rep. 2024;14(1):18996. doi: https://doi.org/10.1038/s41598-024-70270-4