
 UK
UK  EN
EN 

Tongshun Cheng1
![]() Nazia Feroze *1
Nazia Feroze *1
![]() Muhammad Sabil Farooq2
Muhammad Sabil Farooq2
![]()
Key words: interpretive bias, smokers, smoker identity, contextual interventions, psychological interventions
Ключові слова: інтерпретаційне упередження, курці, ідентичність курця, контекстні втручання, психологічні втручання
Abstract
Smoking-related interpretive bias, a core aspect of cognitive distortion in addiction, remains poorly understood regarding its specific characteristics and underlying activation mechanisms. This study addressed this gap through three sub studies exploring the intrinsic properties of smokers’ interpretive bias, the role of smoker identity, and the moderating effect of cognitive load. The Ambiguous Scenario Test was employed to assess interpretive bias. Results revealed that smokers exhibited significantly higher levels of smoking related interpretive bias compared to nonsmokers. Furthermore, smokers with a strong smoker identity displayed more pronounced bias than those with a weak identity. Importantly, the predictive influence of smoker identity on this bias diminished as cognitive load increased, indicating that cognitive resources modulate the identity bias relationship. These findings suggest that sufficient cognitive capacity is necessary for smoker identity to effectively activate associated interpretive biases. By clarifying the core features of smoking-related interpretive bias, identifying smoker identity as a key contributor, and demonstrating cognitive load’s moderating role, this research advances theoretical understanding of cognitive bias components and triggering mechanisms in smokers. The results also hold practical implications for developing targeted interventions aimed at disrupting maladaptive cognitive processes in smoking behavior.
Реферат
Реконфігурація когнітивного упередження в курців: інтегрований підхід, що поєднує ідентичність і контекстуальні втручання. Ченг Тонгшун, Фероз Назія, Фарук Мухаммад Сабіль. Інтерпретаційне упередження, пов’язане з курінням, яке є ключовим аспектом когнітивних викривлень при залежності, залишається недостатньо вивченим з точки зору його специфічних характеристик і механізмів активації. Це дослідження заповнює зазначену прогалину шляхом проведення трьох піддосліджень, спрямованих на вивчення внутрішніх властивостей інтерпретаційного упередження в курців, ролі ідентичності курця та модераторного ефекту когнітивного навантаження. Для оцінювання інтерпретаційного упередження було використано тест неоднозначних сценаріїв (Ambiguous Scenario Test). Результати показали, що курці демонструють значно вищий рівень інтерпретаційного упередження, пов’язаного з курінням, порівняно з некурцями. Крім того, у курців з вираженою ідентичністю курця це упередження проявляється сильніше, ніж в осіб зі слабкою ідентичністю. Важливо зазначити, що прогностичний вплив ідентичності курця на вираженість цього упередження зменшувався зі зростанням когнітивного навантаження, що свідчить про роль когнітивних ресурсів у модерації зв’язку між ідентичністю та інтерпретаційним упередженням. Ці результати вказують на те, що для ефективної активації відповідних інтерпретаційних упереджень ідентичності курця необхідний достатній рівень когнітивних ресурсів. Уточнюючи ключові характеристики інтерпретаційного упередження, пов’язаного з курінням, визначаючи ідентичність курця як важливий чинник і демонструючи модераторну роль когнітивного навантаження, це дослідження розширює теоретичне розуміння компонентів когнітивних упереджень і механізмів їх активації в курців. Отримані результати також мають практичне значення для розроблення цільових втручань, спрямованих на переривання дезадаптивних когнітивних процесів, що лежать в основі поведінки куріння.
Reducing national smoking prevalence and modifying smokers’ behavior remain central goals of tobacco control policies in China. Previous research indicates that smokers often display cognitive biases when processing smoking-related cues, which reinforce smoking behavior and hinder quitting [40, 41]. These biases play a key role in addiction persistence and smoking cessation failure [8]. Cognitive biases include attentional, memory, and interpretive bias [25], but existing studies focus primarily on attentional bias [44], with limited attention to interpretive bias. Interpretive bias is the tendency to select a specific explanation for ambiguous information, reflecting a systematic preference [22]. Unlike attentional bias, it occurs later in cognitive processing and directly reflects how individuals assign meaning to situations [28], making it critical for understanding smokers’ cognitive processes. Research on interpretive bias in addiction has focused on alcohol use. Woud et al. (2012) developed a measure using ambiguous scenarios; heavy drinkers interpreted them more often in alcohol-related ways than light drinkers [42], a pattern confirmed in alcohol-dependent individuals [43]. Like alcohol addiction, smoking stems from physiological and psychological responses to substances, but smokers face more frequent cue exposure: they typically smoke 10-20 cigarettes daily [47] and often carry cigarettes. Thus, investigating smoking-related interpretive bias is vital. Hypothesis 1: Smokers show significantly higher smoking-related interpretive bias than nonsmokers. Theories explaining interpretive bias in addiction include Incentive Sensitization Theory (Robinson, Berridge) [34], Dual Process Model (Salemink, Wiers) [36], and Cognitive Mechanisms of Addiction [10], collectively suggesting smokers may exhibit biased processing of smoking cues. Addiction cues integrate with self-concept to form an addict identity (Frings, Albery) [16]; smoker identity is the degree to which individuals incorporate the smoker role into their self-concept [14]. Though unstudied directly, smoker identity influences smoking behaviors [3, 5, 6, 26], and identity shapes cognitive biases in other domains [1, 13, 21, 29, 39]. Hypothesis 2: Smokers with stronger smoker identity show higher smoking-related interpretive bias. Schema Theory (Beck, Haigh) [2] and the Self-Reference Effect [45, 46] suggest smoker identity guides interpretive processing. Cognitive load may moderate this relationship: high cognitive load reduces reflective processing resources [12, 23, 37]. Hypothesis 3: The effect of smoker identity on smoking-related interpretive bias weakens as cognitive load increases.
The purpose of this study is to examine the characteristics and mechanisms of smoking related interpretive bias among smokers. Specifically, the study investigates differences in interpretive bias between smokers and nonsmokers, examines the influence of smoker identity on interpretive bias, and explores the moderating role of cognitive load in this relationship. To achieve these objectives, three sub studies were conducted. Study 1 compared interpretive bias between smokers and nonsmokers. Study 2 manipulated smoker identity using a social identity salience paradigm to examine its influence on interpretive bias. Study 3 introduced a cognitive load manipulation using a digit memory task to investigate the moderating role of cognitive resources.
MATERIALS AND METHODS OF RESEARCH
Study 1: Characteristics of smokers’ smoking related interpretive bias
Sample size was calculated using G*Power 3.1.9.7 software, with an effect size of 0.25, α error probability of 0.05, and statistical power of 0.80, requiring a minimum of 34 participants. Participants were recruited through online social platforms such as WeChat, resulting in 40 smokers and 40 nonsmokers. Eligibility criteria for smokers were: 1) Daily smoking with a minimum of 5 cigarettes per day; 2) No major physical or mental illnesses, and no history of other substance addictions. After all participants completed the experiment, 5 invalid participants with a scenario judgment accuracy rate below 80% in the interpretive bias test were excluded, leaving 75 valid participants. Among them, there were 36 smokers (all male) and 39 nonsmokers (38 males, 1 female), with average ages of 23.61 years (SD=2.72) and 23.59 years (SD=2.67), respectively no significant difference was found (t (73)=0.03, p=0.973). For smokers, the average age of first smoking was 17.97 years (SD=2.35), average smoking duration was 5.62 years (SD=2.60), average daily smoking quantity was 11.36 cigarettes (SD=7.64), average nicotine dependence score was 3.08 (SD=2.25), and average smoking craving score was 3.71 (SD=1.73).
A 2 (Participant Type: Smoker, Nonsmoker) × 2 (Interpretation Target Sentence Type: Smoking related, smoking unrelated) mixed experimental design was used. Participant type was a between subjects’ variable, interpretation target sentence type was a within subject’s variable, and the dependent variable was interpretive bias.
(1) Measure of interpretive bias: Referring to the experimental materials used in a series of alcohol related interpretive bias studies by Woud et al. [42, 43], 24 smoking related ambiguous scenarios were compiled (each with 2 interpretation target sentences). Thirty postgraduate students majoring in psychology rated the scenarios on theme relevance, interpretive fluency, and valence, and provided revision suggestions, leading to the final selection of 9 ambiguous scenarios. Each scenario was paired with two interpretation target sentences: one smoking related and one smoking unrelated. For example, the scenario was: “You walk restlessly in the room. You are dissatisfied with the current situation you have a backlog of work, and now you’ve lost your wallet. You just want to forget all the…” The two interpretation target sentences were: “You want to forget all your troubles and decide to smoke a cigarette” and “You want to forget all your troubles and decide to go for a run.” Participants were asked to rate the degree of fit between the behavior described in each interpretation target sentence and the scenario (1=Very inconsistent, 4=Very consistent).
(2) Nicotine Dependence Scale: The Fagerström Test for Nicotine Dependence (Heatherton et al.) [20] was used. The scale consists of 6 items (e.g., “Over the past month, how many cigarettes have you smoked per day?”). Scores were converted and summed, with higher scores indicating greater nicotine dependence. The internal consistency coefficient (Cronbach’s α) of the scale in this study was 0.75.
(3) Smoking Craving Scale: The Brief Questionnaire of Smoking Urges (Cox et al.) [11] was used. The scale includes 10 items (e.g., “I really want to smoke a cigarette now”), rated on a 7 point scale (1=completely disagree, 7=completely agree). Higher scores indicate stronger smoking craving. The internal consistency coefficient (Cronbach’s α) of the scale in this study was 0.95.
(4) Self compiled demographic questionnaire: The questionnaire included gender, age, history of organic brain diseases and mental illnesses, and history of other substance addictions. Smokers were also asked to report their age of first smoking and average daily smoking quantity.
The overall experimental procedure was as follows: 1) One day before the experiment, smokers were prescreened online and scheduled for the experiment. To control pre experimental smoking craving, they were instructed not to smoke within 2 hours before the experiment [24, 48]. 2) Upon arriving at the laboratory, participants were informed of the experimental process and precautions. 3) Participants completed the informed consent form, demographic questionnaire, Nicotine Dependence Scale, and Smoking Craving Scale. 4) Both smoker and nonsmoker groups completed the same interpretive bias test. 5) After the experiment, participants were paid and thanked.
The interpretive bias test procedure referred to Woud et al. [43]. Participants completed 9 ambiguous scenario tasks. The procedure for each scenario is shown in Figure 1: 1) Presentation of the ambiguous scenario, with the last character of the final sentence omitted. 2) Participants were asked to fill in the missing character according to the context. 3) Feedback was provided: if correct, the complete character was displayed in green; if incorrect, a red error message appeared, prompting participants to retry. 4) After each scenario, a question asking whether participants understood the scenario’s meaning was presented, and participants responded “Correct” or “Incorrect.” 5) The ambiguous scenario and its two interpretation target sentences were presented again, and participants rated the fit between each target sentence and the scenario.
Statistical analysis was conducted using the Statistical Package for the Social Sciences software, version 26.0 (SPSS Inc., Chicago, IL, USA; license number Z12345678). Before the main analysis, data quality was assessed. Participants whose character completion accuracy rate was lower than 80 percent were excluded from further analysis to ensure data reliability. Quantitative data are presented as median and interquartile range. Qualitative variables are presented as frequencies and percentages where appropriate. The interpretive bias scores were calculated by averaging participants’ responses to the interpretation target sentences across nine ambiguous scenarios. Two scores were obtained for each participant, namely the smoking related interpretive bias score and the smoking unrelated interpretive bias score. To examine differences between groups and interpretation types, repeated measures analysis of variance was applied. Group membership served as the between subject factor, while interpretation type served as the within subject factor. Statistical procedures were performed according to established statistical methodology described in standard statistical literature (Field, 2018). The level of statistical significance was set at p<0.05. Reference for statistical methods: Field A. Discovering Statistics Using IBM SPSS Statistics. 5th ed. London: SAGE Publications; 2018.
The flowchart includes fixation point (1000 ms), scenario presentation (5000 ms), character filling (5000 ms), feedback (3000 ms), scenario judgment, and evaluation stages. Example scenario and target sentences are as described above.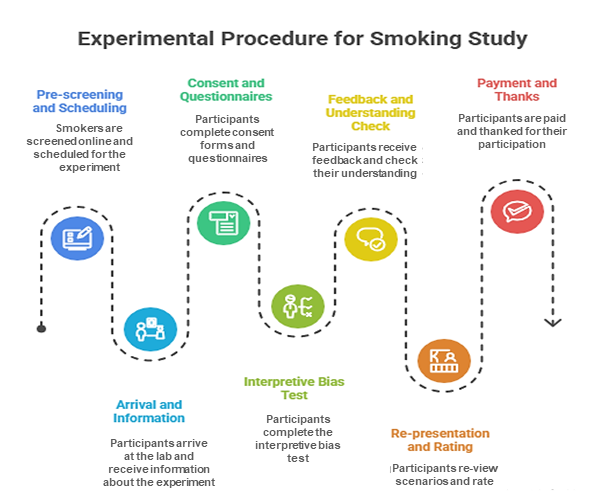
The research was conducted in accordance with the principles of bioethics set out in the WMA Declaration of Helsinki – “Ethical principles for medical research involving human participants” and “Universal Declaration on Bioethics and Human Rights” (UNESCO).
RESULTS AND DISCUSSION
The smoking related and smoking unrelated interpretive bias scores of participants in Study 1 are shown in Figure 2. Repeated measures ANOVA on interpretive bias scores revealed a significant main effect of participant type (F (1,73)=88.00, p<0.001, partial η²=0.55), with nonsmokers showing significantly lower interpretive bias than smokers. A significant main effect of interpretation target sentence type was also found (F (1, 73)=58.15, p<0.001, partial η²=0.44), with participants exhibiting significantly higher interpretive bias for smoking unrelated sentences than smoking related sentences. The interaction between participant type and interpretation target sentence type was significant (F (1, 73)=133.61, p<0.001, partial η²=0.65).
Simple effects analysis showed that for smoking related sentences, smokers’ interpretive bias scores (M=3.01, SD=0.32) were significantly higher than those of nonsmokers (M=1.62, SD=0.55) (F (1, 73)=175.85, p<0.001, partial η²=0.71). For smoking unrelated sentences, there was no significant difference between smokers (M=2.78, SD=0.38) and nonsmokers (M=2.73, SD=0.38) (F (1, 73)=0.31, p=0.578). Additionally, for smokers, interpretive bias scores for smoking related sentences (M=3.01, SD=0.32) were significantly higher than those for smoking unrelated sentences (M=2.78, SD=0.38) (F (1, 73)=7.44, p=0.008, partial η²=0.09). For nonsmokers, interpretive bias scores for smoking related sentences (M=1.62, SD=0.50) were significantly lower than those for smoking unrelated sentences (M=2.73, SD=0.38) (F (1, 73)=191.69, p<0.001, partial η²=0.72).
* – p<0.05, *** – p<0.001: the same applies below.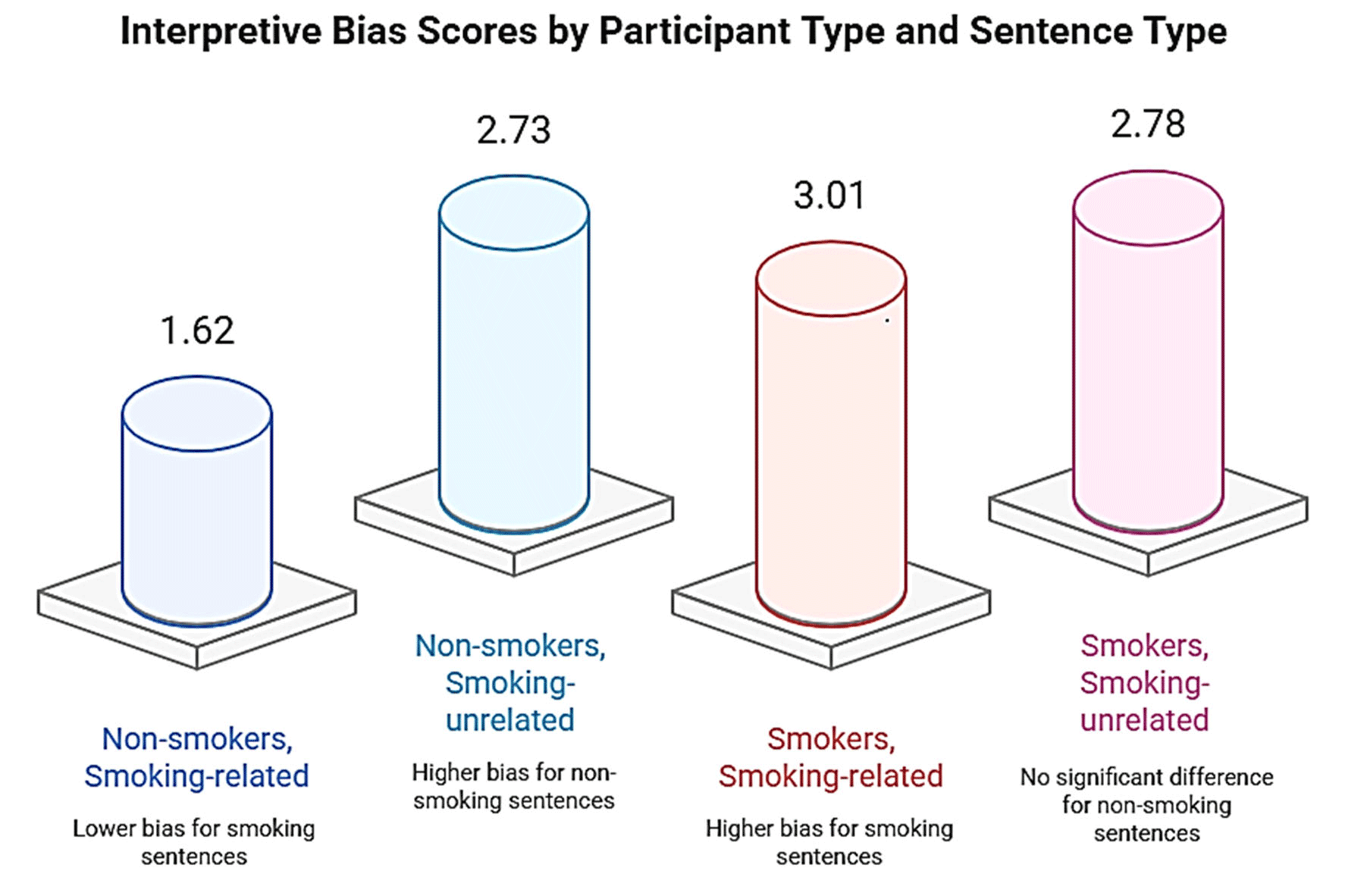
Study 2: The Effect of Smoker Identity on Smokers’ Interpretive Bias
Sample size was calculated using G*Power 3.1.9.7 software, with an effect size of 0.25, α error probability of 0.05, and statistical power of 0.80, requiring a minimum of 34 participants. A total of 66 smokers were recruited through online social platforms, with the same eligibility criteria as Study 1. Participants were randomly assigned to the high smoker identity group or the low smoker identity group. Four invalid participants with a scenario judgment accuracy rate below 80% in the interpretive bias test were excluded, leaving 62 valid participants (49 male, 13 female). The high smoker identity group included 31 participants (26 male, 5 female), and the low smoker identity group included 31 participants (23 male, 8 female). There were no significant differences between the two groups in average age (20.84 years, SD=2.34 vs. 21.32 years, SD=1.85; t(60)=0.91, p=0.370), age of first smoking (17.42 years, SD=1.57 vs. 17.03 years, SD=1.72; t(60)=1.29, p=0.201), smoking duration (3.42 years, SD=2.42 vs. 4.29 years, SD=2.08; t(60)=1.51, p=0.135), average daily smoking quantity (8.26 cigarettes, SD=3.37 vs. 8.71 cigarettes, SD=3.86; t(60)=0.49, p=0.625), nicotine dependence (2.81, SD=1.70 vs. 3.45, SD=1.61; t(60)=1.53, p=0.130), or smoking craving (4.17, SD=1.19 vs. 4.52, SD=1.10; t(60)=1.20, p=0.237).
A 2 (Smoker Identity Group: High, Low) × 2 (Interpretation Target Sentence Type: Smoking related, smoking unrelated) mixed experimental design was used. Smoker identity was a between subject’s variable, interpretation target sentence type was a within subject’s variable, and the dependent variable was interpretive bias.
(1) Measure of interpretive bias: same as study 1.
(2) Materials for manipulating smoker identity: the social identity salience paradigm (Haslam et al.) [19] was used. In the high smoker identity group, participants were asked to write three things for each of the following four scenarios: “Three things you often do with most of your smoking friends or important members of the smoking group,” “Three things you and most of your smoking friends or important members of the smoking group rarely do,” “Three things you and most of your smoking friends or important members of the smoking group do well,” and “Three things you and most of your smoking friends or important members of the smoking group do not do well.” In the low smoker identity group, participants were asked to write three things for each of the following four scenarios: “Three things you often do,” “Three things you rarely do,” “Three things you do well,” and “Three things you do not do well.”
(3) Smoker Identity Scale: The Smoker Self Identity Scale (Moan, Rise) [31] was used. The scale includes 4 items (e.g., “I consider myself a smoker”), rated on a 7 point scale (1= completely inconsistent, 7= completely consistent). Higher scores indicate stronger identification with the smoker identity. The internal consistency coefficient (Cronbach’s α) of the scale in this study was 0.75.
(4) Other measures: Nicotine Dependence Scale, Smoking Craving Scale, and demographic questionnaire were the same as in Study 1.
The overall experimental procedure was as follows: 1) One day before the experiment, smokers were prescreened online or by phone and instructed not to smoke within 2 hours before the experiment. 2) Upon arriving at the laboratory, participants were informed of the experimental process and precautions. 3) Participants completed the informed consent form, demographic questionnaire, Nicotine Dependence Scale, and Smoking Craving Scale. 4) Participants were randomly assigned to the high or low smoker identity group and completed the corresponding identity manipulation task. 5) Participants completed the manipulation check for smoker identity. 6) Participants completed the interpretive bias test. 7) After the experiment, participants were paid and thanked.
Data processing was similar to Study 1, with the addition of one sample t tests and independent samples t tests to verify the effectiveness of the smoker identity manipulation.
Effectiveness of smoker identity manipulation
One sample t tests were used to examine the difference between each group’s smoker identity level and the midpoint (5.13). The results showed that the low smoker identity group’s score (M=4.39, SD=0.82) was significantly lower than the midpoint (t(30)=5.05, p<0.001), while the high smoker identity group’s score (M=6.13, SD=0.44) was significantly higher than the midpoint (t(30)=12.72, p<0.001). Independent samples t tests revealed that the high smoker identity group had significantly higher smoker identity scores than the low smoker identity group (t(60)=10.45, p<0.001, Cohen’s d=2.65). These results confirm the effectiveness of the smoker identity manipulation.
The effect of smoker identity on interpretive bias
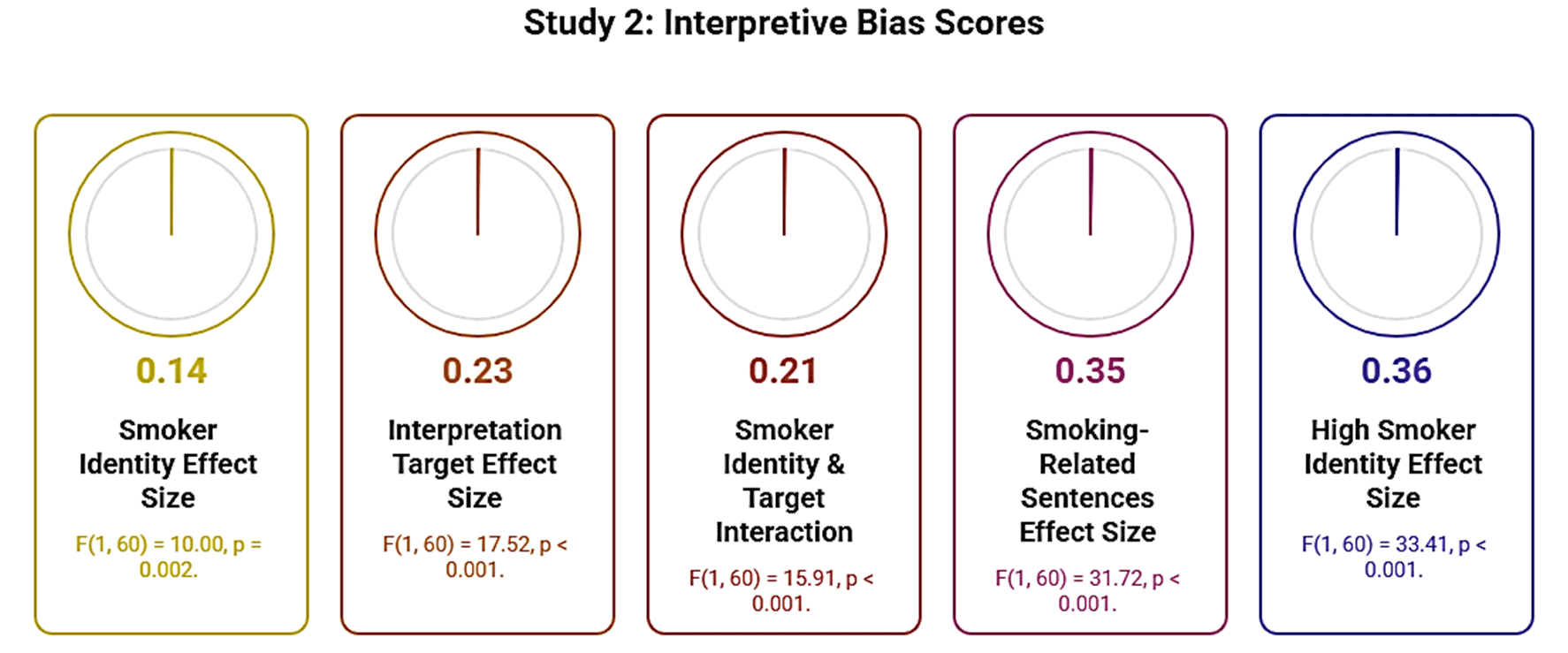
The smoking related and smoking unrelated interpretive bias scores of participants in Study 2 are shown in Figure 3. Repeated measures ANOVA on interpretive bias scores revealed a significant main effect of smoker identity (F (1, 60)=10.00, p=0.002, partial η²=0.14), with the low smoker identity group showing significantly lower interpretive bias than the high smoker identity group. A significant main effect of interpretation target sentence type was found (F (1, 60)=17.52, p<0.001, partial η²=0.23), with participants exhibiting significantly higher interpretive bias for smoking related sentences than smoking unrelated sentences. The interaction between smoker identity and interpretation target sentence type was significant (F (1, 60)=15.91, p<0.001, partial η²=0.21). Simple effects analysis showed that for smoking related sentences, the high smoker identity group’s interpretive bias scores (M=3.44, SD=0.25) were significantly higher than those of the low smoker identity group (M=2.88, SD=0.49) (F (1, 60)=31.72, p<0.001, partial η²=0.35). For smoking unrelated sentences, there was no significant difference between the high smoker identity group (M=2.84, SD=0.53) and the low smoker identity group (M=2.86, SD=0.44) (F (1, 60)=0.03, p=0.862). Additionally, for the high smoker identity group, interpretive bias scores for smoking related sentences (M=3.44, SD=0.25) were significantly higher than those for smoking unrelated sentences (M=2.84, SD=0.53) (F (1, 60)=33.41, p<0.001, partial η²=0.36). For the low smoker identity group, there was no significant difference between interpretive bias scores for smoking related sentences (M=2.88, SD=0.49) and smoking unrelated sentences (M=2.86, SD=0.44) (F (1, 60)=0.02, p=0.890).
Study 3: The Effect of Smoker Identity on Smokers’ Interpretive Bias: The Role of Cognitive Load
Sample size was calculated using G*Power 3.1.9.7 software, with an effect size of 0.25, α error probability of 0.05, and statistical power of 0.80, requiring a minimum of 24 participants. A total of 64 smokers were recruited through online social platforms, with the same eligibility criteria as Study 1. Participants were randomly assigned to the high smoker identity group or the low smoker identity group. Four invalid participants with a scenario judgment accuracy rate below 80% in the interpretive bias test were excluded, leaving 60 valid participants (50 male, 10 female). The high smoker identity group included 30 participants (25 male, 5 female), and the low smoker identity group included 30 participants (25 male, 5 female). There were no significant differences between the two groups in average age (21.17 years, SD=2.87 vs. 20.97 years, SD=1.56; t(58)=0.34, p=0.738), age of first smoking (17.20 years, SD=1.75 vs. 16.93 years, SD=2.00; t(58)=0.55, p=0.585), smoking duration (3.97 years, SD=3.27 vs. 4.03 years, SD=2.09; t(58)=0.09, p=0.925), average daily smoking quantity (8.10 cigarettes, SD=5.33 vs. 8.57 cigarettes, SD=4.58; t(58)=0.36, p=0.717), nicotine dependence (3.83, SD=1.80 vs. 4.07, SD=1.23; t(58)=0.59, p=0.560), or smoking craving (4.72, SD=1.08 vs. 4.96, SD=0.57; t(58)=1.09, p=0.283).
A 2 (Smoker Identity Group: High, Low) × 2 (Interpretation Target Sentence Type: Smoking related, smoking unrelated) × 2 (Cognitive Load: High, Low) three factor mixed experimental design was used. Smoker identity was a between subject’s variable, while interpretation target sentence type and cognitive load were within subject’s variables. The dependent variable was interpretive bias.
(1) Measure of interpretive bias: Same as Study 1.
(2) Materials for manipulating smoker identity and Smoker Identity Scale: Same as Study 2.
(3) Materials for manipulating cognitive load and manipulation check: The cognitive load manipulation tool developed by Drichoutis and Nayga [12] was used, involving memorizing random numbers of different lengths. High cognitive load materials consisted of 7 digit random numbers (e.g., “1473268”), while low cognitive load materials consisted of 2 digit random numbers (e.g., “41”). The manipulation check questionnaire for cognitive load included 3 items: “How much mental effort did you invest in the number string memory task? (1= none at all, 7= All effort)”, “I did not have enough mental capacity to carefully consider my decisions. (1= completely disagree, 7= completely agree)”, and “The number string memory task distracted me while making decisions (1= completely disagree, 7= completely agree)”.
(4) Other measures: Nicotine Dependence Scale, Smoking Craving Scale, and demographic questionnaire were the same as in Study 1.
The overall experimental procedure was as follows: 1) One day before the experiment, daily smokers were prescreened online or by phone and instructed not to smoke within 2 hours before the experiment. 2) Upon arriving at the laboratory, participants were informed of the experimental process and precautions. 3) Participants completed the informed consent form, demographic questionnaire, Nicotine Dependence Scale, and Smoking Craving Scale. 4) Participants were randomly assigned to the high or low smoker identity group, completed the corresponding identity manipulation task, and filled out the manipulation check questionnaire for smoker identity. 5) Participants completed the cognitive load manipulation task (high or low, counterbalanced to control for order effects), followed by the cognitive load manipulation check questionnaire. 6) Participants completed the interpretive bias test. 7) Participants completed the other cognitive load manipulation task (low or high) and the corresponding manipulation check questionnaire. 8) Participants completed the interpretive bias test again. 9) After the experiment, participants were paid and thanked.
Data processing was similar to Study 2, with the addition of a manipulation check for cognitive load.
Effectiveness of Smoker Identity Manipulation
One sample t tests were used to examine the difference between each group’s smoker identity level and the midpoint (5.38). The results showed that the low smoker identity group’s score (M=4.47, SD=0.87) was significantly lower than the midpoint (t(29)=5.73, p<0.001), while the high smoker identity group’s score (M=6.11, SD=0.42) was significantly higher than the midpoint (t(29)=9.53, p<0.001). Independent samples t tests revealed that the high smoker identity group had significantly higher smoker identity scores than the low smoker identity group (t(58)=9.29, p<0.001, Cohen’s d=2.40). These results confirm the effectiveness of the smoker identity manipulation.
Effectiveness of Cognitive Load Manipulation
Paired samples t tests were used to examine differences in cognitive load levels between the two conditions. The results showed that participants’ scores under high cognitive load (M=5.23, SD=1.84) were significantly higher than those under low cognitive load (M=3.21, SD=1.00) (t(59)=19.03, p<0.001, Cohen’s d=1.64). These results confirm the effectiveness of the cognitive load manipulation.
The Effects of Smoker Identity and Cognitive Load on Interpretive Bias
The smoking related and smoking unrelated interpretive bias scores of participants in Study 3 are shown in Figure 4. Repeated measures ANOVA on interpretive bias scores revealed a significant main effect of smoker identity (F (1, 58)=9.77, p=0.003, partial η²=0.14), with the low smoker identity group showing significantly lower interpretive bias than the high smoker identity group. A significant main effect of interpretation target sentence type was found (F (1, 58)=29.40, p<0.001, partial η²=0.34), with participants exhibiting significantly higher interpretive bias for smoking related sentences than smoking unrelated sentences. The main effect of cognitive load was not significant (F (1, 58)=2.80, p=0.100). The interaction between smoker identity and interpretation target sentence type was significant (F (1, 58)=5.28, p=0.025, partial η²=0.08). The interaction between smoker identity and cognitive load was significant (F (1, 58)=7.78, p=0.007, partial η²=0.12). The interaction between interpretation target sentence type and cognitive load was not significant (F (1, 58)=2.79, p=0.100). The three way interaction was marginally significant (F (1, 58)=3.35, p=0.073, partial η²=0.06).
Simple effects analysis showed that for smoking related sentences: under low cognitive load, the high smoker identity group’s interpretive bias scores (M=3.55, SD=0.36) were significantly higher than those of the low smoker identity group (M=3.07, SD=0.43) (F (1, 58)=21.27, p<0.001, partial η²=0.27); under high cognitive load, the high smoker identity group’s scores (M=3.44, SD=0.39) were still significantly higher than those of the low smoker identity group (M=3.18, SD=0.51) (F (1, 58)=4.97, p=0.030, partial η²=0.08), but the significance was reduced. For smoking unrelated sentences: under low cognitive load, there was no significant difference between the high smoker identity group (M=2.84, SD=0.36) and the low smoker identity group (M=2.83, SD=0.38) (F (1, 58)=0.04, p=0.848); under high cognitive load, there was also no significant difference between the two groups (M=2.90, SD=0.35 vs. M=2.93, SD=0.44) (F (1, 58)=0.06, p=0.801).
This study conducted three sub studies to investigate the characteristics of smokers’ smoking related interpretive bias, the effect of smoker identity on this bias, and the moderating role of cognitive load. Study 1 showed that smokers exhibited significantly higher smoking related interpretive bias than nonsmokers. Study 2 revealed that smokers with high smoker identity had significantly stronger smoking related interpretive bias than those with low smoker identity. Study 3 found that the effect of smoker identity on smoking related interpretive bias diminished as cognitive load increased.
Regarding the characteristics of smokers’ interpretive bias, this study confirms that smokers exhibit interpretive bias toward smoking related cues, supporting Hypothesis 1. Similar results have been found in other substance addiction research, particularly among drinkers [37, 42, 43]. For example, heavy drinkers are more likely to interpret alcohol related ambiguous scenarios in alcohol related ways than light drinkers [42]. Possible reasons for smokers’ smoking related interpretive bias include: First, the association between cues and automatic responses. According to the Incentive Sensitization Theory [34] and the Dual Process Model [36], repeated exposure to smoking related cues leads to the formation of automatic cue response associations in smokers, which triggers smoking related interpretive bias when facing smoking related stimuli or situations. Second, the impact of cues on cognitive function. According to the Cognitive Mechanisms of Addiction model [10], smoking related cues or situations activate smokers’ existing smoking related implicit cognition and impair the metacognitive system and executive function that monitor smoking behavior, leading to cognitive biases. Third, the role of rationalization beliefs. According to the theory of smoking rationalization beliefs [7], smokers are often aware of the health risks of smoking, which creates a conflict with their actual smoking behavior. This conflict causes discomfort, prompting smokers to form rationalization beliefs to reduce discomfort these beliefs may enhance or induce smoking related interpretive bias.
Regarding the inducing factors of smokers’ smoking related interpretive bias, this study shows that smoker identity induces such bias, supporting Hypothesis 2. Similar findings have been reported in other fields on the effect of identity on cognitive bias [1, 27]. For example, individuals’ identification with the vegetarian identity increases their attentional bias toward healthy food related cues [1]. Possible mechanisms underlying the effect of identity on smoking related interpretive bias include: First, the salience of smoker identity activates the association between the self and smoking. In fact, smokers have multiple identities [30], and when the smoker identity is salient, the association between the self and smoking is activated [17]. Due to the self-relevant information processing advantage effect [46], individuals may interpret ambiguous information based on the framework of the self-smoking association. Second, smoker identity activates positive attitudes toward smoking and cognition of smoking benefits. Through long term exposure to cigarettes and the pleasant experiences derived from smoking, smokers have formed positive evaluations and attitudes toward smoking [33]. According to Schema Theory (Beck, Haigh) [2], when processing ambiguous situations in depth, smokers are more likely to process information consistent with existing smoking related schemas in memory. Identity salience activates these evaluations and attitudes, providing a content basis for interpreting ambiguous information. Third, smoker identity activates smoking action schemas. Smoking action schemas include processes related to smoking behavior, such as the actions from lighting a cigarette to smoking [32]. Smoking is a hallmark behavior of smokers, and the salience of the smoker identity may activate these action schemas. According to Schema Theory [2], activated smoking action schemas or schema sets may combine with current ambiguous information, providing a content basis for smoking related interpretive bias.
Regarding the moderating role of cognitive load in the relationship between smoker identity and smoking related interpretive bias, this study shows that the effect of smoker identity decreases as cognitive load increases, supporting Hypothesis 3. This result indicates that sufficient cognitive resources enhance the effect of smoker identity on smoking related interpretive bias. Possible mechanisms include: First, processing information activated by identity may require cognitive resources. Identity provides relevant information for interpretive bias, and this information may be processed through two pathways [23, 30, 37]: automatic processing and controlled processing. Under high cognitive load, automatic processing of smoking related information is activated; under low cognitive load, sufficient cognitive resources support controlled processing of smoking related information. Second, processing information required for interpretive bias requires cognitive resources. The activation of smoker identity brings information about smoking identity, the pros and cons of smoking, and smoking actions. According to the Cognitive Mechanisms of Addiction model (Copersino, 2017), sufficient cognitive resources facilitate the full processing of this information particularly the effective retrieval, encoding, comparison, organization, sorting, and evaluation of relevant information, all of which require cognitive resources. Third, effective interpretive bias requires inhibiting interference from irrelevant information. According to the Cognitive Mechanisms of Addiction model [10], interpretive bias may be interfered with by irrelevant information, and inhibiting such interference requires cognitive resources. For smokers, information related to other identities (e.g., occupational identity) is also stored in long term memory and may interfere with smoking related interpretive bias suppressing this interference requires cognitive resources.
This study makes several theoretical contributions: First, by examining the characteristics of smokers’ smoking related interpretive bias, it expands the understanding of the components of smokers’ cognitive biases and broadens the explanatory scope of the Incentive Sensitization Theory, Dual Process Model, and Cognitive Mechanisms of Addiction model. Second, by demonstrating the inducing effect of smoker identity on smoking related interpretive bias, it enriches research on the influencing factors of smokers’ interpretive bias, supplements previous theories emphasizing the role of cue response associations (e.g., Incentive Sensitization Theory), and provides a new perspective for understanding the psychosocial mechanisms of addicts’ interpretive bias from a social cognitive orientation. Third, by revealing the moderating role of cognitive load, it enriches empirical research on the effect of identity on smoking related responses, identifies potential conditions for the effect of identity on interpretive bias, supplements previous theories explaining identity mechanisms (e.g., Schema Theory), and provides evidence for interpreting the mechanism of identity’s effect on interpretive bias based on the Dual Process Model.
This study also has practical implications for reducing national smoking rates and smokers’ smoking behavior in China: First, for the government, it is necessary to continue strictly implementing smoke free policies and expanding smoke free environments. This not only promotes smokers to restructure their interpretations of smoking related situations but also increases situations that induce nonsmoker identities, thereby reducing smoking related interpretive bias. Second, for media campaigns: on the one hand, smoking related scenes in film and television works should be strictly prohibited; on the other hand, advertisements promoting alternative interpretations of smoking related situations should be increased, helping smokers understand that common situations can be interpreted from multiple perspectives (e.g., stress can be relieved through deep breathing, exercise, or venting, not just smoking). Third, for clinical practitioners involved in smoking cessation interventions: when helping smokers quit, attention should be paid to correcting their smoking related interpretive bias. During correction, smokers’ “smoker identity” should be transformed into “ex-smoker identity” or “nonsmoker identity.” At the same time, smokers should be guided to allocate more cognitive resources to problem solving rather than smoking related content when facing difficulties, thereby preventing the activation of smoking related interpretive bias by smoker identity. Fourth, for smokers themselves: increasing interactions with nonsmokers or successful quitters can reduce smoker identity, helping them learn to view situations perceived as closely related to smoking from multiple angles and ultimately reducing smoking related interpretive bias.
This study has several limitations: First, the participants were all young smokers. Compared with middle aged and elderly smokers, young smokers have shorter smoking durations and lower nicotine dependence. Future research should compare the characteristics of smoking related interpretive bias among smokers with different smoking durations. Second, this study used behavioral experiments. Future research can combine cognitive neuroscience techniques to explore the neural mechanisms underlying the effects of smoker identity and cognitive load on smoking related interpretive bias. Third, in the laboratory setting, smokers were aware they were participating in an experiment, which may have led them to anticipate cues and affect experimental validity. Future research can use more ecologically valid methods such as ecological momentary assessment to study the effect of identity on interpretive bias. Fourth, smoking related interpretive bias does not necessarily translate into actual smoking behavior. The process by which cognitive bias influences behavior may be affected by numerous factors, and future research should further explore the specific psychological processes through which smoking related interpretive bias translates into smoking behavior.
CONCLUSION
1. In summary, this study investigated the characteristics, triggering factors, and moderating mechanisms of smokers’ smoking-related interpretive bias through three sequential sub-studies. Results confirmed that smokers demonstrate significantly higher smoking-related interpretive bias than non-smokers, supporting the extension of addiction cognitive theories to smoking behavior.
2. Additionally, smokers with a strong smoker identity exhibit more pronounced smoking-related interpretive bias compared to those with a weak identity, highlighting smoker identity as a key psychosocial trigger for this cognitive distortion.
3. Critically, cognitive load moderates the relationship between smoker identity and interpretive bias: the facilitating effect of smoker identity diminishes under high cognitive load, indicating that sufficient cognitive resources are necessary for identity to activate smoking-related interpretive bias.
4. These findings advance theoretical understanding of smokers’ cognitive biases by integrating social identity and cognitive resource perspectives, while offering practical implications for tobacco control.
5. Interventions targeting smoking cessation could focus on reshaping smoker identity and guiding cognitive resource allocation to reduce maladaptive interpretive tendencies, complementing existing tobacco control strategies.
Contributors:
Cheng Tongshun – conceptualization, methodology, supervision, funding acquisition;
Feroze Nazia – data curation, formal analysis, investigation, writing – original draft;
Farooq Muhammad Sabil – resources, validation, writing – review & editing.
Funding. This study was supported by the National Social Science Foundation of China (Grant No.: 22BSH089) and the Tianjin Social Science Foundation (Grant No.: TJSR2023-005).
Conflict of interests. The authors declare no conflict of interest.
REFERENCES
Albery IP, Shove E, Bartlett G, Frings D, Spada MM. Individual differences in selective attentional bias for healthy and unhealthy food-related stimuli and social identity as a vegan/vegetarian dissociate “healthy” and “unhealthy” orthorexia nervosa. Appetite. 2022;178:106261. doi: https://doi.org/10.1016/j.appet.2022.106261- Beck AT, Haigh EA. Advances in cognitive theory and therapy: The generic cognitive model. Annu Rev Clin Psychol. 2014;10(1):1-24. doi: https://doi.org/10.1146/annurev-clinpsy-032813-153734
- Callaghan L, Yong HH, Borland R, Cummings KM, Hitchman SC, Fong GT. What kind of smoking identity following quitting would elevate smokers’ relapse risk? Addict2021;112:106654. doi: https://doi.org/10.1016/j.addbeh.2020.106654
- Cao M, Xie P, Sun L, Zhang J, Kong F, Zhou Z. Processing priority for avatar reference in online games: Evidence from behavioral and ERP studies. Acta Psychol Sin.2021;53(6):639-50. doi: https://doi.org/10.3724/SP.J.1041.2021.00639
- Chen H, Fan Y, Li X, Gao L, Li W. The relationship between smoker identity and smoking cessation among young smokers: The role of smoking rationalization beliefs and cultural value of guanxi. Front Psychiatry. 2022;13:812982. doi: https://doi.org/10.3389/fpsyt.2022.812982
- Chen H, Wang Y, Zhao B, Yao J, Li W. Identity and smoking refusal self-efficacy in Chinese male smokers: The mediating role of smoking refusal outcome expectancies and the moderating role of social norms. J Psychol2023;46(6):1504-10. doi: https://doi.org/10.16719/j.cnki.1671-6981.20230618
- Chen H, Yang Y, Zheng E, Fan Y, Gao L. Smokers’ “bulletproof vest”: The formation mechanism and interventions of self-exempting beliefs. Adv Psychol Sci. 2024;32(4):654-63. doi: https://doi.org/10.3724/SP.J.1042.2024.00654
- Cheng J, Guan Y, Zhang Y, Bi Y, Bu L, Li Y, et al. Electrophysiological mechanisms of biased response to smoking-related cues in young smokers. Neurosci Lett. 2016;629:85-91. doi: https://doi.org/10.1016/j.neulet.2016.06.044
- Chu J, Pink SL, Willer R. Religious identity cues increase vaccination intentions and trust in medical experts among American Christians. Proc Natl Acad Sci U S A. 2021;118(49):e2106481118. doi: https://doi.org/10.1073/pnas.2106481118
- Copersino ML. Cognitive mechanisms and therapeutic targets of addiction. Curr Opin Behav Sci. 2017;13:91-8. doi: https://doi.org/10.1016/j.cobeha.2016.11.005
- Cox LS, Tiffany ST, Christen AG. Evaluation of the brief questionnaire of smoking urges (QSU-brief) in laboratory and clinical settings. Nicotine Tob Res. 2001;3(1):7-16. doi: https://doi.org/10.1080/14622200124218
- Drichoutis AC, Nayga RM Jr. Economic rationality under cognitive load. Econ J. 2020;130(632):2382-409. doi: https://doi.org/10.1093/ej/ueaa070
- Dunham Y, Emory J. Of affect and ambiguity: The emergence of preference for arbitrary ingroups. J Soc Issues.2014;70(1):81-98. doi: https://doi.org/10.1111/josi.12060
- Falomir-Pichastor JM, Blondé J, Desrichard O, Felder M, Riedo G, Folly L. Tobacco dependence and smoking cessation: The mediating role of smoker and ex-smoker self-concepts. Addict Behav. 2020;102:106200. doi: https://doi.org/10.1016/j.addbeh.2019.106200
- Feng Z, Zhang D, Yang G. Recalling, recognition, and priming processing in middle school students with depressive symptoms. Acta Psychol Sin. 2008;40(2):166-74. doi: https://doi.org/10.3724/SP.J.1041.2008.00166
- Frings D, Albery IP. The social identity model of cessation maintenance: Formulation and initial evidence. Addict2015;44:35-42. doi: https://doi.org/10.1016/j.addbeh.2015.01.007
- Grigutsch LA, Lewe G, Rothermund K, Koranyi N. Implicit “wanting” without implicit “liking”: A test of incentive sensitization theory in the context of smoking addiction using the wanting implicit association test (W-IAT). J Behav Ther Exp Psychiatry. 2019;64:9-14. doi: https://doi.org/10.1016/j.jbtep.2019.05.002
- Haslam C, Haslam SA, Jetten J, Cruwys T, Steffens NK. Life change, social identity, and health. Annu Rev2021;72(1):635-61. doi: https://doi.org/10.1146/annurev-psych-122419-033451
- Haslam SA, Oakes PJ, Reynolds KJ, Turner JC. Social identity salience and the emergence of stereotype consensus. Pers Soc Psychol Bull. 1999;25(7):809-18. doi: https://doi.org/10.1177/0146167299025007004
- Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström test for nicotine dependence: A revision of the Fagerström Tolerance Questionnaire. BrJ 1991;86(9):1119-27. doi: https://doi.org/10.1111/j.1360-0443.1991.tb01879.x
- Hehman E, Mania EW, Gaertner SL. Where the division lies: Common ingroup identity moderates the cross-race facial recognition effect. J Exp Soc Psychol. 2010;46(2):445-8. doi: https://doi.org/10.1016/j.jesp.2009.11.007
- Hirsch CR, Clark DM, Mathews A. Imagery and interpretations in social phobia: Support for the combined cognitive biases hypothesis. Behav Ther. 2006;37(3):223-36. doi: https://doi.org/10.1016/j.beth.2006.02.002
- Hofmann W, Friese M, Wiers RW. Impulsive versus reflective influences on health behavior: A theoretical framework and empirical review. Health Psychol Rev. 2008;2(2):111-37. doi: https://doi.org/10.1080/17437190802617668
- Huijding J, de Jong PJ, Wiers RW, Verkooijen K. Implicit and explicit attitudes toward smoking in a smoking and a nonsmoking setting. Addict Behav. 2005;30(5):949-61. doi: https://doi.org/10.1016/j.addbeh.2004.09.020
- Jones A, Field M. Does cognitive bias modification reduce alcohol consumption? In: Cooke R, Conroy D, Davies EL, Hagger MS, de Visser RO, editors. The Palgrave handbook of psychological perspectives on alcohol consumption. Cham: Springer International Publishing; 2021. p. 527-50. doi: https://doi.org/10.1007/978-3-030-66941-6_24
- Kale D, Jackson S, Brown J, Garnett C, Shahab L. Social smoker identity and associations with smoking and quitting behaviour: A cross-sectional study in England. DrugAlcohol 2024;260:111345. doi: https://doi.org/10.1016/j.drugalcdep.2024.111345
- Lakritz C. When control over food spirals out of control: Investigating the cognitive mechanisms of food hyper-selectivity in individuals suffering from anorexia nervosa and orthorexia nervosa [doctoral dissertation]. [Internet]. Lyon: Université Claude Bernard Lyon 1; 2023 [cited 2025 Dec 23]. Available from: https://hal.science/tel-04449969v1/file/Final_Manuscrit_Lakritz_Clara_pour_impression.pdf
- Li T, Feng F. Interpretation bias in social anxiety: Research paradigms, characteristics and modification. Adv Psychol2013;21(12):2196-203. doi: https://doi.org/10.3724/SP.J.1042.2013.02196
- Liang M, Zhao Y, Yin C. Common ingroup identity promotes ethnic psychological compatibility: The mediating role of positive interpretation bias. J Psychol Sci. 2023;46(2):386-93. doi: https://doi.org/10.16719/j.cnki.1671-6981.20230214
- Lindgren KP, Neighbors C, Gasser ML, Ramirez JJ, Cvencek D. A review of implicit and explicit substance self-concept as a predictor of alcohol and tobacco use and misuse. Am J Drug Alcohol Abuse. 2017;43(3):237-46. doi: https://doi.org/10.1080/00952990.2016.1213272
- Moan IS, Rise J. Quitting smoking: Applying an extended version of the theory of planned behavior to predict intention and behavior. J Appl Biobehav Res. 2005;10(1):39-68. doi: https://doi.org/10.1111/j.1751-9861.2005.tb00006.x
- Motschman CA, Tiffany ST. Cognitive regulation of smoking behavior within a cigarette: Automatic and nonautomatic processes. Psychol Addict Behav. 2016;30(4):494-9. doi: https://doi.org/10.1037/adb0000160
- Poole R, Carver H, Anagnostou D, Edwards A, Moore G, Smith P, et al. Tobacco use, smoking identities and pathways into and out of smoking among young adults: A meta-ethnography. Subst Abuse Treat Prev Policy. 2022;17:24. doi: https://doi.org/10.1186/s13011-022-00448-9
- Robinson TE, Berridge KC. The neural basis of drug craving: An incentive-sensitization theory of addiction. BrainRes 1993;18(3):247-91. doi: https://doi.org/10.1016/0165-0173(93)90013-P
- Roccas S, Brewer MB. Social identity complexity. Pers Soc Psychol Rev. 2002;6(2):88-106. doi: https://doi.org/10.1207/S15327957PSPR0602_01
- Salemink E, Wiers RW. Adolescent threat-related interpretive bias and its modification: The moderating role of regulatory control. Behav Res Ther. 2012;50(1):40-6. doi: https://doi.org/10.1016/j.brat.2011.10.006
- Salemink E, Woud ML, Roos M, Wiers R, Lindgren KP. Reducing alcohol-related interpretive bias in negative affect situations: Using a scenario-based cognitive bias modification training paradigm. Addict Behav. 2019;88:106-13. doi: https://doi.org/10.1016/j.addbeh.2018.08.028
- Sritharan R, Gawronski B. Changing implicit and explicit prejudice. Soc Psychol. 2010;41(3):113-23. doi: https://doi.org/10.1027/1864-9335/a000017
- Wang X, Zhu J, Liu L, Chen X. Cognitive processing bias in Chinese student teachers with strong and weak professional identity. Front Psychol. 2017;8:784. doi: https://doi.org/10.3389/fpsyg.2017.00784
- Wilcockson TD, Pothos EM, Osborne AM, Crawford TJ. Top-down and bottom-up attentional biases for smoking-related stimuli: Comparing dependent and nondependent smokers. Addict Behav. 2021;118:106886. doi: https://doi.org/10.1016/j.addbeh.2021.106886
- Wittekind CE, Schiebel T, Kühn S. Reliability of and associations between cognitive bias measures and response inhibition in smoking. J Behav Ther Exp Psychiatry. 2023;81:101853. doi: https://doi.org/10.1016/j.jbtep.2023.101853
- Woud ML, Fitzgerald DA, Wiers RW, Rinck M, Becker ES. “Getting into the spirit”: Alcohol-related interpretation bias in heavy drinking students. Psychol Addict Behav.2012;26(3):627-32. doi: https://doi.org/10.1037/a0028142
- Woud ML, Becker ES, Rinck M, Salemink E. The relationship between drinking motives and alcohol-related interpretation biases. J Behav Ther Exp Psychiatry. 2015;47:102-10. doi: https://doi.org/10.1016/j.jbtep.2014.12.004
- Xia X, Wang D, Li Y, Zhu X, Tan X, Wu Y. The trial-by-trial fluctuations in primary motor cortex excitability during attentional bias among smokers: A transcranial magnetic stimulation study. Int J Clin Health Psychol. 2024;24(2):100468. doi: https://doi.org/10.1016/j.ijchp.2024.100468
- Xin C, Chen Y, Tian M, Liu G. The self-reference effect in prospective memory and its cognitive mechanisms in elementary school students aged 7 to 11 years. Acta Psychol Sin. 2025;57(5):775-91. doi: https://doi.org/10.3724/SP.J.1041.2025.00775
- Yang H, Wang F, Gu N, Huang X. Processing priority for self-related information: Evidence from visual search of screen names. Acta Psychol Sin. 2012;44(4):489-97. doi: https://doi.org/10.3724/SP.J.1041.2012.00489
- Yu J, Cui Z, Pan L, Sun J, Cao Y, Wang Y, et al. Smoking prevalence among 20-80-year-old Han residents in urban and rural regions of Hebei province. Chin J Public Health.2022;38(1):61-4. doi: https://doi.org/10.11847/zgggws1134589
- Zhao B, Chen H. Effects of smoking social cues on inhibitory control in smokers: An event-related potential study. Int J Clin Health Psychol. 2023;23(4):100387. doi: https://doi.org/10.1016/j.ijchp.2023.100387