
 UK
UK  EN
EN 

M.Z. Vorobets
![]() D.Z. Vorobets
D.Z. Vorobets
![]() R.V. Fafula
R.V. Fafula
![]() O.V. Melnyk
O.V. Melnyk
![]() N.E. Lychkovska
N.E. Lychkovska
![]() Z.D. Vorobets *
Z.D. Vorobets *
![]() O.M. Chemerys
O.M. Chemerys
![]()
Key words: premature ejaculation, erectile dysfunction, combat injury, venlafaxine, dapoxetine
Ключові слова: передчасна еякуляція, еректильна дисфункція, бойова травма, венлафаксин, дапоксетин
Abstract
Premature ejaculation is one of the most common male sexual disorders and occurs with a frequency of 21-33% in various populations. The etiology of premature ejaculation is practically not established, although it is a fairly common type of sexual dysfunction. According to various data, sexual dysfunction occurs in 49.1-80% veterans of combat-actions with post-traumatic stress disorder. Premature ejaculation can interfere with sexual satisfaction, leading to a reduced quality of life for men and their partners. It has been shown that serotonin reuptake inhibitors may be the drugs of choice in the treatment of premature ejaculation. The aim of the work was to improve methods of treating sexual dysfunction accompanied by premature ejaculation in men injured as a result of hostilities. 56 men injured as a result of hostilities with sexual dysfunction and complaints of premature ejaculation were examined. Patients were divided into two groups depending on the selected selective serotonin reuptake inhibitors – venlafaxine (n=24) and dapoxetine (n=32) which they had been receiving for at least 1.5 months. After treatment with both serotonin reuptake inhibitors, reactive and personality anxiety symptoms objectively decreased, as assessed by the Spielberger-Hanan scale. Treatment with venlafaxine and paroxetine resulted in a significant reduction in depressive symptoms in men with premature ejaculation. They turned out to be relatively balanced drugs with satisfactory efficacy and relatively few side effects. However, venlafaxine, compared to dapoxetine, produced 2.1 times fewer side effects and 20% fewer relapses. The average duration of sexual intercourse after treatment with both drugs positively correlated with the overall improvement of sexual function according to the IIEF-5 scale (r=0.70; p<0.05 for the first group; r=0.85; p<0.05 for the second group). An inverse correlation was found between the average duration of sexual intercourse and the score of anxiety symptoms on the Spielberger-Hanin scale in patients of both study groups (r= -0.69; p<0.05 for the first group; r= -0.68; p<0.05 for the second group). Although dapoxetine is considered the “gold standard” among serotonin reuptake inhibitors for the treatment of premature ejaculation, the drug is used by the patient only on demand, and other drugs in this group, which are antidepressants, may have a more positive effect on patients with depression and concomitant premature ejaculation, who have suffered as a result of hostilities. The study demonstrates that the neurotransmitter serotonin plays a key role in the modulation of ejaculation, as the use of its reuptake inhibitors, in particular dapoxetine and venlafaxine, contributes to an increase in intravaginal latency time to ejaculation.
Реферат
Порівняльний ефект дапоксетину та венлафаксину в лікуванні передчасної еякуляції чоловіків, постраждалих унаслідок бойових дій. Воробець М.З., Воробець Д.З., Фафула Р.В., Мельник О.В., Личковська Н.Е., Воробець З.Д., Чемерис О.М. Передчасна еякуляція є одним з найбільш поширених чоловічих статевих розладів і зустрічається з частотою 21-33% у різних популяціях. Етіологія передчасної еякуляції практично не встановлена, хоча вона є досить поширеним видом сексуальної дисфункції. За різними даними, у ветеранів бойових дій із посттравматичним стресовим розладом сексуальна дисфункція зустрічається в 49,1-80%. Передчасна еякуляція може перешкоджати сексуальному задоволенню, що призводить до зниження якості життя чоловіків та їхніх партнерок. Показано, що саме інгібітори зворотного захоплення серотоніну можуть бути препаратами вибору при лікуванні передчасної еякуляції. Метою роботи було удосконалення методів лікування статевої дисфункції, що супроводжується передчасною еякуляцією, у чоловіків, постраждалих унаслідок бойових дій. Обстежено 56 чоловіків, постраждалих унаслідок бойових дій, із сексуальною дисфункцією та скаргами на передчасну еякуляцію. Пацієнтів розподілено на дві групи залежно від вибраного препарату селективного інгібітора зворотного захоплення серотоніну, який вони отримували щонайменше 1,5 місяці: венлафаксин (n=24) та дапоксетин (n=32). Після лікування обома інгібіторами зворотного захоплення серотоніну в чоловіків об’єктивно зменшилась реактивна та особистісна тривожна симптоматика, яка оцінювалась за шкалою Спілбергера-Ханана. Лікування венлафаксином і дапоксетином привело до вірогідного зменшення депресивної симптоматики в чоловіків з передчасною еякуляцією. Вони виявились відносно збалансованими препаратами із задовільною ефективністю і відносно невеликою кількістю побічних ефектів. Однак дапоксетин, порівняно з венлафаксином, давав у 2,1 раза меншу кількість побічних ефектів і на 20% менше рецидивів. Середня тривалість статевого акту після лікування обома препаратами позитивно корелює із загальним покращенням сексуальної функції за шкалою МІЕФ-5 (r=0,70; p<0,05 для першої групи; r=0,85; p<0,05 для другої групи). Обернена кореляція виявлена між середньою тривалістю статевого акту та балом тривожної симптоматики за шкалою Спілбергера-Ханіна в пацієнтів обох досліджуваних груп (r= -0,69; p<0,05 для першої групи; r= -0,68; p<0,05 для другої групи). Хоча «золотим стандартом» серед препаратів інгібіторів зворотного захоплення серотоніну для лікування передчасної еякуляції вважається дапоксетин, препарат вживається пацієнтом лише за вимогою, а інші препарати цієї групи, які відносяться до антидепресантів, можуть мати також позитивний вплив саме на пацієнтів з депресією та супутньою передчасною еякуляцією, постраждалих унаслідок бойових дій. Дослідження демонструє, що нейротрансмітер серотонін відіграє ключову роль у модуляції еякуляції, оскільки застосування інгібіторів його зворотного захоплення, зокрема дапоксетину та венлафаксину, сприяє збільшенню інтравагінального латентного часу до настання еякуляції.
Men with sexual dysfunction often complain of premature ejaculation (PE) which is considered as the inability to control ejaculation for “enough” time to have sexual intercourse [1, 2, 3]. Premature ejaculation is one of the most common male sexual disorders and occurs with a frequency of 21-33% in different populations [2, 4]. According to other data, 25-40% of men in the USA suffer from PE [5, 6]. The etiology of PE is practically not established, although it is a fairly common type of sexual dysfunction.
According to various data, sexual dysfunction occurs in 49.1-80% of combat veterans with posttraumatic stress disorder [7, 8, 9]. PE can interfere with sexual satisfaction, leading to a decrease in the life quality of patients and their partners [1, 3]. The mechanism of PE development is not fully understood, especially considering the role of physiological mechanisms of action of selective serotonin reuptake inhibitors (SSRI). SSRI were introduced into the treatment of PE after psychopharmacological studies on the pathways of ejaculation control [1, 2, 10].
Psychological factors often influence the occurrence of PE. Men sometimes underestimate the connection between sexual ability and emotional well-being. PE can be caused by temporary depression or stress. However, it is often necessary to use drugs that slow down the rate of arousal. Serotonin reuptake inhibitors have been indicated as the drugs of choice in the treatment of PE [1-5]. Along with behavioral therapy, this paper presents our comparative experience with the use of medications in this group. Clinical and laboratory studies of sexual dysfunction in recent years have led to the development of new treatment protocols, including psychosexual and local negative pressure therapy methods, and new pharmacological drugs [1, 3, 11].
Dapoxetine hydrochloride, a short-acting selective serotonin reuptake inhibitor, is currently the only oral drug recommended on label [1, 2, 12-15]. The mechanism of action of dapoxetine in PE is likely related to the inhibition of serotonin reuptake by neurons and the subsequent enhancement of the effects of neurotransmitters on pre- and postsynaptic receptors. Analysis of clinical studies has confirmed that this on-demand treatment improves the quality of life of the patient and his sexual partner [1, 10]. However, the drug is taken only on demand, and is often viewed by patients as a "one-off", that is, one that does not treat the causes of the disease and cannot potentially cure it. Dapoxetine causes the most significant delay in ejaculation among SSRI, which are antidepressants, and is therefore widely used for the treatment of PE [18]. Although dapoxetine was originally developed as an antidepressant, it has been largely unused for the treatment of depression and is now only used for the treatment of PE [19].
Patients who have suffered as a result of hostilities and who are consulted by a psychiatrist often exhibit depressive symptoms and are prescribed antidepressants. Some of the antidepressants that belong to the SSRI group also have a positive effect on prolonging the intravaginal latency time before ejaculation. Therefore, one drug can be successfully used by a psychiatrist and a sexologist to treat depression and concomitant PE.
Venlafaxine is an antidepressant from the group of selective serotonin and norepinephrine reuptake inhibitors, also used to treat PE [16, 17].
All forms of ejaculatory disorders require a comprehensive psychological examination of patients using objective questionnaire methods, and the development of modern comprehensive therapy methods, which will ensure better cure rates. In this study, we sought to evaluate the treatment effect of dapoxetine compared with venlafaxine on combat veterans with combat injuries accompanied by depressive and sexual disorders, in particular PE in real-world practice and to investigate factors influencing treatment effectiveness. The aim of the work was to improve methods of treating sexual dysfunction accompanied by premature ejaculation in men injured as a result of hostilities.
MATERIALS AND METHODS OF RESEARCH
The research was conducted at the Urology Clinic of the Danylo Halytsky Lviv National Medical University and the Military Medical Clinical Hospital in the Western Region. The work was based on the results of the examination and treatment of 56 men injured as a result of hostilities, with sexual dysfunction and complaints of premature ejaculation. The age of the patients ranged from 20 to 53 years, with a mean age of 39±5.2 years. All patients completed and signed an informed consent to participate in the studies. The research was carried out in compliance with all principles of medical ethics and protection of patients' rights, human dignity and moral and ethical norms, in accordance with the principles of the Helsinki Declaration of Human Rights, the Council of Europe Convention on Human Rights and Biomedicine, the Laws of Ukraine that determine this; permission of the Bioethics Commission of the Danylo Halytskyi Lviv National Medical University (protocol No. 7 of 26.06.2023).
All patients underwent a questionnaire based on the IIEF-5 scale (International Index of Erectile Function-5) [20, 21], a sexological and urological history was collected, a rectal examination of the prostate was performed, microscopy of the prostate secretion for the presence of an inflammatory process, prostate ultrasonography, and, if indicated, bacteriological culture of the prostate secretion, and, if necessary, PCR diagnostics of the relevant pathogens in the prostate secretion.
To determine health-related quality of life (QOL), a survey was conducted using the SF-36 questionnaire [22, 23, 24]. According to the etiological principle, neurogenic genesis of PE was found among all examined patients. Patients were routinely consulted by a psychologist, sexologist, and psychiatrist. The main complaint of patients was PE, which persisted with regular sexual activity 2.4±0.3 times/week. Patients were assigned to this group in the absence of complaints, anamnesis, clinical, instrumental and laboratory data of the presence of prostatitis (colliculoprostatitis) or chronic pelvic pain syndrome. All patients of this group had a pathological fixation on sexual dysfunction, which was accompanied by an affective component in the form of anxiety, fear of failure, bad mood, and intense doubts, and led to the dominance of the sympathetic nervous system during sexual intimacy [1, 11, 12]. The average duration of the disease was 9.0±0.8 months.
Thus, the study group included only men with neurogenic (psychogenic) PE, which in all 56 (100%) occurred after a combat injury (multiple shrapnel and bullet wounds). Given the complexity of the pathogenesis of PE, the treatment of all patients was comprehensive and consisted of two parts: basic therapy and selective serotonin reuptake inhibitors (SSRI).
Patients were divided into two groups depending on the chosen SSRI drug, which they received for at least 1.5 months: group 1 (n=24) received venlafaxine, 37.5-150 mg/day; group 2 (n=32) received dapoxetine, 30-60 mg/day.
To objectively reflect anxiety and depression, patient questionnaires were used using the Spielberger-Hanin and Hamilton scales, respectively [24]. During the treatment process, criteria for determining erectile dysfunction were taken into account.
To assess the effectiveness of treatment methods for patients with ejaculatory disorders, the obtained digital data were processed by statistics methods using parametric and nonparametric multiple comparison methods. The results are presented as arithmetic means with standard errors (M±m) and medians with 25% and 75% percentiles (Me [Q25; Q75]). The reliability of differences between independent quantitative variables with a normal distribution was assessed using the Student (t) and Mann-Whitney U-test. Differences between the study groups were considered statistically significant at p<0.05. The correlation was calculated by determining the Spearman's rank correlation coefficient [24, 25]. Mathematical processing of the results was carried out using the application package of licensed statistical program Microsoft Excel (Microsoft Office Standard 00218-04988-70316-AA857).
RESULTS AND DISCUSSION
Treatment of men with premature ejaculation was included in the study. Men with sexual dysfunction usually have impaired sexual motivation: instead of focusing on the process of lovemaking, patients are focused on the fact that sexual intercourse may end prematurely. They experience tension and anxiety instead of positive emotions. Given this, an important component of the success of the treatment was the patient's ability to learn to clearly navigate their feelings and apply a functional training option in a timely manner in order to prevent the ejaculatory reflex from being triggered. The effectiveness of PE treatment in patients of both SSRI groups, expressed in an increase in the duration of sexual intercourse (IELT), the presence and severity of side effects, as well as PE recurrences, is shown in Table.
Thus, before the start of treatment, the average duration of sexual intercourse in group 1 was 1.0±0.4 minutes. In all 24 patients of group 1, therapy was initiated with a dose of venlafaxine 37.5 mg in the evening for 2-4 days, followed by a transition to 37.5 mg twice a day to prevent nausea, which was observed with varying severity up to the first 5 days of administration in 16/24 (66.7%), and then completely disappeared in 22/24 men. One patient refused to continue using the drug.
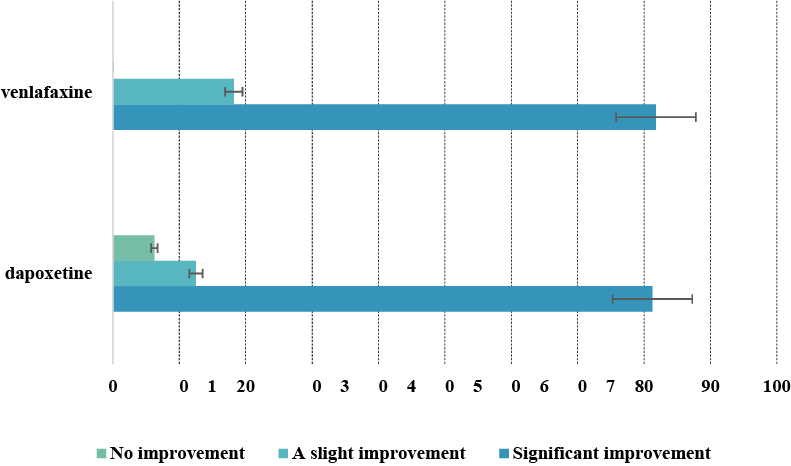
Most patients experienced moderate general weakness and fatigue a few days after the start of treatment, which was difficult to objectify due to the significant polymorphism of subjective sensations. Moderate decreased libido and mild erectile dysfunction were noted by 8/24 (33%) men. The positive side is the rapid increase of the intravaginal latency time to ejaculation (IELT) within 5-7 days of taking venlafaxine. The negative side is that the drug is the most expensive in the SSRI segment. By 1.5 months of treatment, 18/22 (81.8%) men reported significant subjective improvement with an average increase in IELT of 3.0±0.45 min; two others (18.2%), not satisfied with the duration of IELT, switched to a dose of 150 mg twice a day and after 2 weeks reported an IELT of 5.0±0.12 min. Therefore, the overall effectiveness of venlafaxine in patients of our clinic was almost 100% and depended only on the dose received. However, the recurrence of PE after drug withdrawal was 18/24 (75%). Some patients indicated a positive effect (increased IELT) from taking venlafaxine "on demand", a few hours before the expected sexual intercourse, but these data cannot be reliably objectified. 10/24 (41.7%) patients agreed to continue taking venlafaxine after 1.5 months.
In group 2, before the start of treatment, the average duration of sexual intercourse was 1.0±0.4 min. In all 32 patients in group 2, therapy was initiated with a dose of dapoxetine 20 mg/day in the afternoon, preferably after work, for 45 days, which was well tolerated. Among the side effects during the first few days of taking the drug, the most common were nausea, dizziness, headache, and diarrhea for 1-3 days in 10/32 (31.25%) men, which usually resolved quickly. Moderate decreased libido and mild erectile dysfunction were noted by 8/32 (25%) men. After 1.5 months, 26/32 (81.25%) men reported significant subjective improvement with an average increase in IELT to 3.0±0.34 min; 4/32 (12.5%) reported slight improvement with IELT to 2±0.12 min, and 2/32 (6.25%) reported no increase in the duration of sexual intercourse with IELT of 1.0±0.03 min.
Groups > group 1 (n=24) venlafaxine 75 mg/day group 2 (n=32) dapoxetine 30 mg/day Treatment > until after until after Average duration of sexual intercourse (intravaginal latency time to ejaculation (IELT)), min, (M±m, Me[Q25; Q75]) 1.0±0.4 1.2 [0.8; 1.3] 3.0±0.45* 3.4 [3.2; 3.7] (81.8% - significant improvement) 5.0±0.12* 4.9 [4.8; 5.1] (18.2% - significant improvement after increasing the dose 1.0±0.4 1.2 [0.8; 1.3] 3.0±0.34* 3.3 [3.0; 3.8] (81.25% - significant improvement) 2.0±0.12* 2.1 [2.0; 2.3] (12.5% - slight improvement after increasing the dose 1.0±0.03 1.0 [1.0; 1.1] (6.25% - no improvement) total efficiency 93.75% Adverse effects, % 66.70 31.25 Decreased libido and mild ED, % 33 25 Overall improvement in sexual performance on the IIEF scale across all domains, number of points 5.4 6.2 Depressive symptoms according to the Hamilton scale, points 6 5 6 5 Anxiety symptoms according to the Spielberger-Hanin scale, reactive/personal, scores 34/31 15/9* 34/31 15/9* Patients who wish to continue treatment for more than 1.5 months, % 41.70 43.75 PE recurrence after drug withdrawal, % 75.0 62.5 Notes: * the difference with the indicator before treatment is significant, p<0.05.
to 150 mg/d) total efficiency 100%
to 40 mg/d)
The latter agreed to increase the dose of paroxetine to 40 mg/day over the next month. Only five (31.25%) men who experienced significant improvement and two (12.5%) who noted moderate improvement – a total of 43.75% patients decided to continue treatment with paroxetine for more than 1.5 months, explaining this by the same reluctance to commit to systematic pill use. Different respondents noted an increase in IELT from 1 week to 1 month of dapoxetine use. Episodic use of this drug did not lead to a significant prolongation of the duration of coitus. The recurrence of PE from the first days of drug withdrawal to six months was 20/32 (62.5%). Overall, patients were fairly satisfied with dapoxetine, given its average effectiveness, average cost, and minor side effects compared to other SSRI.
Overall, the results obtained indicate the effectiveness of treating PE with serotonin reuptake inhibitors (Fig. 1).
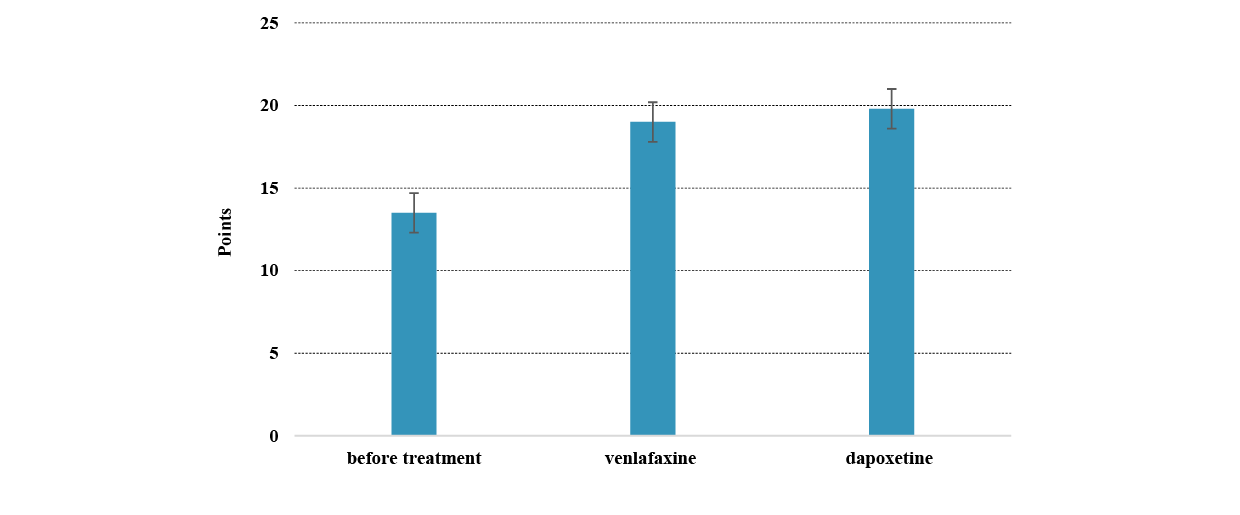
The vast majority of patients ultimately found medication treatment psychologically difficult, as it only helps with systematic use and does not provide a lasting effect after discontinuation. The fact that the total IIEF-5 score increased by 5.4 and 6.2 after treatment with venlafaxine and paroxetine, respectively, turned out to be interesting (Fig. 2).
This once again indicates the close relationship between all components of sexual function, when, with the improvement of the ability to control ejaculation, the scores of the IIEF domains, which reflect the improvement of sexual function in general, simultaneously improve. Also, after treatment with SSRI, anxiety in patients with PE significantly decreased, as calculated using the Hamilton scale, which in turn confirms the close relationship between PE, psychogenic symptoms at the clinical level, and the state of serotonergic transmission of excitation at the physiological level. The most pronounced trend towards reduced anxiety is observed after the use of dapoxetine.
After treatment with both SSRI, reactive and personal anxiety symptoms objectively decreased, as assessed by the Spielberger-Hanan scale. However, it is difficult to carry out an absolutely correct comparative analysis of the effectiveness of both drugs, since the groups included men with very different self-assessments of anxiety. Some patients denied it, others noted pronounced anxiety, which was most likely associated with sexual disorders.
Treatment with venlafaxine and dapoxetine resulted in a significant reduction in depressive symptoms in men with PE, but this was more dependent on the even distribution of patient groups, many of whom, despite PE, denied any depression.
Men with PE always hope for a "complete cure," which, unfortunately, is not often possible at current stage of development of sexology, psychiatry, and pharmacology. This necessitates the search for new, more effective treatments.
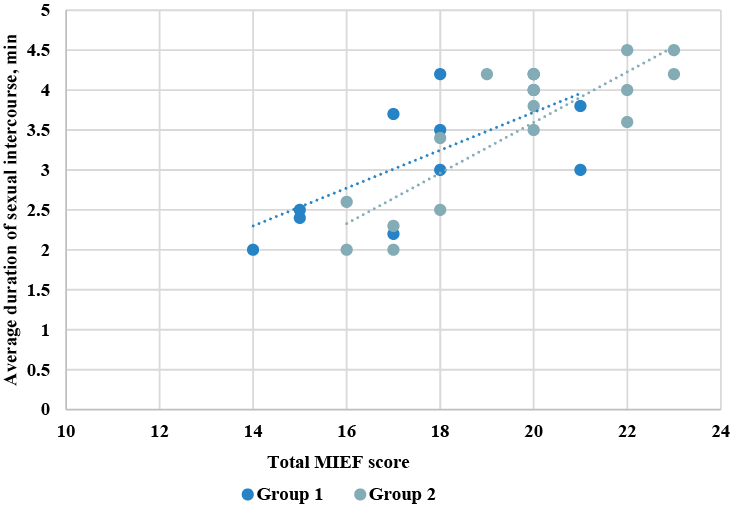
The correlation coefficient was used to determine the relationships between overall improvement in sexual function on the IIEF scale across all domains and average duration of sexual intercourse. The average duration of sexual intercourse after treatment with both drugs is positively correlated with the overall improvement in sexual function according to the
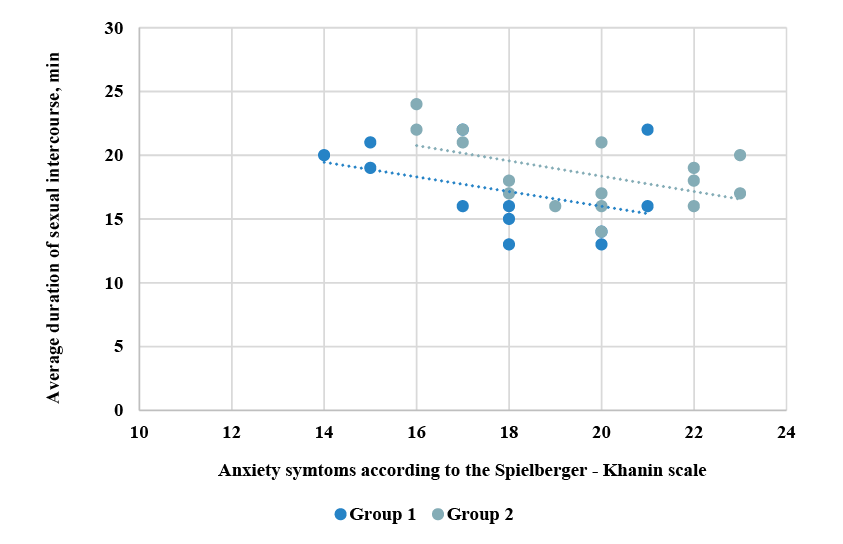
IIEF-5 scale (r=0.70; p<0.05 for the first group; r=0.85; p<0.05 for the second group) (Fig. 3). An inverse correlation was found between the average duration of sexual intercourse and the score of anxiety symptoms on the Spielberger-Hanin scale in patients of both study groups (r= -0.69; p<0.05 for the first group; r= -0.68; p<0.05 for the second group) (Fig. 4).
Thus, the study results indicate an association between combat-related trauma in military personnel and the development of neurogenic (psychogenic) premature ejaculation. According to sexual, urological, and psychoneurological history data, premature ejaculation was not reported prior to participation in combat activities. These results are, to some extent, consistent with those obtained in a study of the impact of stress factors (without injuries) on the civilian population in Israel, resulting from combat operations on sexual dysfunction and, in particular, on PE, which was observed in 56.5% of men [26]. Probably, in our case, the causal pathophysiological relationship between premature ejaculation and the consequences of combat operations is mediated by psychological (stress, anxiety, hyperarousal, development of post-traumatic stress disorder), neurophysiological and hormonal mechanisms, as well as, importantly, by medical treatment of wounds. At the same time, it is obvious that additional research is needed to accurately clarify the mechanisms of premature ejaculation development: psychological, neurophysiological, hormonal, biochemical, and possibly immunological, and others.
The study demonstrates that the neurotransmitter serotonin plays a key role in the modulation of ejaculation, as the use of its reuptake inhibitors promotes the increase in intravaginal latency time to ejaculation.
Among SSRI, venlafaxine and dapoxetine were almost equally effective when used together. However, paroxetine caused significantly fewer side effects (31.25%) compared to venlafaxine (66.7%). Also, dapoxetine resulted in lower recurrence of PE (62.5%) compared to venlafaxine (75.0%). Although, in both cases, after the end of the course of treatment, most patients experienced a recurrence of PE.
The use of selective serotonin reuptake inhibitors leads to an increase in the time to ejaculation [13, 23]. In recent years, the most commonly used drugs for the treatment of PE are Longride, Priligy, and Daporin, but the active ingredient in all of them is Dapoxetine. Before the introduction of dapoxetine, many SSRI were used, but their effectiveness was much lower, since permanent use did not guarantee a stable effect, and long-term use caused the development of side effects [27]. Dapoxetine is the first drug specifically designed for the treatment of PE and has high selectivity [1, 14, 15], although it was primarily developed as an antidepressant [19]. Unlike other SSRI, dapoxetine has no significant clinical electrocardiographic effects, is safe and well tolerated at doses of 30-60 mg/day, although it is prescribed only on demand and cannot potentially cure the psychogenic cause of PE, unlike long-term SSRIs, especially in patients with concomitant depressive symptoms [1].
Some clinical studies previous years indicate of significant efficacy of paroxetine [23, 28, 29]. It has been shown that 77.8% of patients with lifelong PE decided to continue daily dapoxetine use after 3 months of successful use, 30.8% refused due to unsatisfactory efficacy [3, 13].
A multicenter study of married couples over 6 months in 5 countries used stopwatches to measure intravaginal latency time to ejaculation, the period from intromission to ejaculation [3, 30]. It was found that the IELT ranged from 30 seconds to 44 minutes, with an average of 5.4 minutes; also depending on the country – from 3.7 minutes to 7.6 minutes. In more than 14% of men, the average IELT was lower than 200 s, in 26% it was longer than 600 s.
Clomipramine may help in severe cases of PE associated with serious nervous system disorders; the drug has also been reported to improve erection quality in some patients [23]. Intramuscular injections of magnesium sulfate solution have been reported to be successful, as PE is believed to be associated with magnesium deficiency [13, 14]. The use of the LORETA (low-resolution electromagnetic tomography of the brain) functional imaging method in patients revealed that the SSRI sertraline promotes an increase in electrical activity mainly in the frontal, limbic and temporal lobes of the left hemisphere of the brain, which may be associated with the therapeutic effect of SSRI in PE [31, 32, 34].
Some studies have shown that PE in men from different countries of the world occurs even more often than erectile dysfunction, accounting for 20-30% of the population and practically not changing with age [11]. PE not only affects the sexual health of the man, but also negatively affects the psychosocial health of the partner [23, 35].
Due to the polyetiological nature of PE, the involvement in the development of PE of not only anatomical and physiological links of pathogenesis, but also socio-psychological aspects, as well as taking into account the paired nature of sexual function, certain difficulties arise in finding effective comprehensive methods of treating PE at the current stage of development of medicine.
Thus, the study provides new data on the pharmacotherapeutic features of treating premature ejaculation in male combatants with dapoxetine and venlafaxine, contributing to a better understanding of the efficacy and tolerability of selective serotonin reuptake inhibitors in the context of increased anxiety.
CONCLUSIONS
1. Among the serotonin reuptake inhibitors, venlafaxine (100%) was more effective in treating men with premature ejaculation who were injured as a result of combat operations than dapoxetine (93.75%), but no significant difference was found between them (p>0.05).
2. The use of dapoxetine causes fewer side effects (31.25%) in the treatment of premature ejaculation than venlafaxine (66.7%). Also, dapoxetine causes fewer relapses (62.5%), compared to venlafaxine (75%).
3. The average duration of sexual intercourse after treatment of premature ejaculation with dapoxetine and venlafaxine is positively correlated with the overall improvement of sexual function according to the MIEF-5 scale (r=0.70; p<0.05 for the first group; r=0.85; p<0.05 for the second group). An inverse correlation was found between the average duration of sexual intercourse and the score of anxiety symptoms according to the Spielberger-Khanin scale in men of both study groups (r= -0.69; p<0.05 for the first group; r= -0.68; p<0.05 for the second group) injured as a result of hostilities.
4. Due to the absence of a “gold standard” for the treatment of premature ejaculation, dapoxetine and venlafaxine, among selective serotonin reuptake inhibitors, demonstrated comparable efficacy in the treatment of premature ejaculation (with a significant increase in intravaginal ejaculatory latency time) in male combatants, without extrapolation of the results to other therapeutic approaches.
Contributions:
Vorobets M.Z. – treatment, methodology, writing – initial draft;
Vorobets D.Z. – conceptualization, treatment, data curation, writing – review & editing, resources;
Fafula R.V. – formal analysis, verification;
Melnyk O.V. – visualization, formal analysis;
Lychkovska N.E. – visualization;
Vorobets Z.D. – supervision, project administration;
Chemerys O.M. – date curation, project administration.
Funding.The research was conducted with the financial support of a grant from the National Research Foundation of Ukraine “Improving the diagnostics and treatment of sexual and reproductive disorders (disorders) in men affected by hostilities” (registration No. 2022.01/0151).
Conflict of interest. The authors declare no conflict of interest.
REFERENCES
1. Liu G, Yin Y, Zhang L, He D, Yang L. Efficacy of Dapoxetine in the Treatment of Patients With Lifelong Premature Ejaculation as an Alternative to Sertraline Therapy. Sexual Medicine. 2022;10(1):100473. doi: https://doi.org/10.1016/j.esxm.2021.100473
2. Peng J, Fang D, Li H, et al. Efficacy of dapoxetine treatment in Chinese patients with premature ejaculation and possible factors affecting efficacy in the real-world practice. BMC Urol. 2020;20:11. doi: https://doi.org/10.1186/s12894-0200580-3
3. Salonia A, Bettocchi C, Boeri L, Capogrosso P, Carvalho J, Cilesiz NC, et al. European Association of Urology Guidelines on Sexual and Reproductive Health-2021 Update: Male Sexual Dysfunction. Eur Urol. 2021 Sep;80(3):333-57. doi: https://doi.org/10.1016/j.eururo.2021.06.007
4. Gillman N, Gillman M. Premature Ejaculation: Aetiology and Treatment Strategies. Medical Sciences. 2019;7(11):102. doi: https://doi.org/10.3390/medsci7110102
5. Dahm P, Holten M, Ratanawong JP, Lauwagie A, Gonzalez‐Padilla DA. Analysis of European Association of Urology Guidelines 2023 and its adherence to GRADE methodology. Clin Pub Health Guidelines. 2024;1:e70004. doi: https://doi.org/10.1002/gin2.70004
6. Crowdis M, Leslie SW, Nazir S. Premature Ejaculation. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2025 Mar 23]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546701/
7. Bird ER, Piccirillo M, Garcia N, Blais R, Campbell S. Relationship Between Posttraumatic Stress Disorder and Sexual Difficulties: A Systematic Review of Veterans and Military Personnel. J Sex Med. 2021 Aug;18(8):1398-426. doi: https://doi.org/10.1016/j.jsxm.2021.05.011
8. Breyer BN, Fang SC, Seal KH, et al. Sexual Health in Male and Female Iraq and Afghanistan U.S. War Veterans With and Without PTSD: Findings From the VALOR Cohort. Journal of Traumatic Stress. 2016 Jun;29(3):229-36. doi: https://doi.org/10.1002/jts.22097
9. Castillo OJr, Chen IK, Amini E, Yafi FA, Barham DW. Male Sexual Health Related Complications Among Combat Veterans. Sex Med Rev. 2022 Oct;10(4):691-7. doi: https://doi.org/10.1016/j.sxmr.2022.06.002
10. El-Hady AK, El-Gamil DS, Abdel-Halim M, Abadi AH. Advancements in Phosphodiesterase 5 Inhibitors: Unveiling Present and Future Perspectives. Pharmaceuticals (Basel). 2023 Sep 6;16(9):1266. doi: https://doi.org/10.3390/ph16091266
11. DeLay KJ, Haney N, Hellstrom WJ. Modifying Risk Factors in the Management of Erectile Dysfunction: A Review. World J Mens Health. 2016 Aug;34(2):89-100. doi: https://doi.org/10.5534/wjmh.2016.34.2.89
12. Zhong C, Li C, Geng Q, Han Q, Gao Q, Zhang J, et al. Reasons and treatment strategy for discontinuation of dapoxetine treatment in premature ejaculation patients in China: A retrospective observational study. Andrologia. 2022 Aug;54(7):1598-604. doi: https://doi.org/10.1111/and.14425
13. Saleh R, Majzoub A, Abu El-Hamd M. An update on the treatment of premature ejaculation: A systematic review. Arab J Urol. 2021 Aug 4;19(3):281-302. doi: https://doi.org/10.1080/2090598X.2021.1943273
14. Vieiralves RR, Favorito LA. Dapoxetine and premature ejaculation. Int Braz J Urol. 2023 Jul-Aug;49(4):511-4.
doi: https://doi.org/10.1590/S1677-5538.IBJU.2023.9908
15. Tuken M, Culha MG, Serefoglu EC. Efficacy and safety of dapoxetine/sildenafil combination tablets in the treatment of men with premature ejaculation and concomitant erectile dysfunction-DAP-SPEED Study. Int J Impot Res. 2019 Mar;31(2):92-6. doi: https://doi.org/10.1038/s41443-019-0122-2
16. Li J, Liu D, Wu J, Fan X, Dong Q. Dapoxetine for the treatment of premature ejaculation: a meta-analysis of randomized controlled trials with trial sequential analysis. Ann Saudi Med. 2018 Sep-Oct;38(5):366-75. doi: https://doi.org/10.5144/0256-4947.2018.366
17. Ratajczak P, Kus K, Zielińska-Przyjemska M, Skórczewska B, Zaprutko T, Kopciuch D, et al. Antistress and antidepressant properties of dapoxetine and vortioxetine. Acta Neurobiologiae Experimentalis. 2020;80(3):217-24. doi: https://doi.org/10.21307/ane-2020-020
18. Kulacaoglu F. Painful ejaculation induced by venlafaxine: a case report. European Psychiatry. 2022;65(S1):S801-S801. doi: https://doi.org/10.1192/j.eurpsy.2022.2071
19. Liu S, Singh N, Ben W, Mol BW. The integrity of seven randomized trials evaluating treatments for premature ejaculation. Andrologia. 2022;54:e14573. doi: https://doi.org/10.1111/and.14573
20. Quintana GR, Ponce FP, Escudero-Pastén J, Santibáñez-Palma JF, Aguayo-Zuñiga CP, Carrasco-Portiño M, et al. Analysis of the International Index of Erectile Function: psychometric evidence and measurement invariance across relationship status and age generations in a Chilean sample. Sexual Medicine. 2024;12(6): qfae084. doi: https://doi.org/10.1093/sexmed/qfae084
21. Neijenhuijs KI, Holtmaat K, Aaronson NK, Holzner B, Terwee CB, Cuijpers P, et al. The International Index of Erectile Function (IIEF)-A Systematic Review of Measurement Properties. J Sex Med. 2019 Jul;16(7):1078-91. doi: https://doi.org/10.1016/j.jsxm.2019.04.010
22. Lins L, Carvalho FM. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016 Oct 4;4:2050312116671725. doi: https://doi.org/10.1177/2050312116671725
23. Horpinchenko ІІ, Vorobets DZ. [Mechanisms of sexual dysfunction development]. Lviv: LNMU; 2013. 388 p. Ukrainian.
24. Bensken WP, Ho VP, Pieracci FM. Basic Introduction to Statistics in Medicine. Part 2: Comparing Data. Surg Infect (Larchmt). 2021;22(6):597-603. doi: https://doi.org/10.1089/sur.2020.430
25. Pagano M, Gauvreau K, Mattie H. Principles of Biostatistics. CRC Press; 2022. 735 p.
26. Lazar A, Gewirtz-Meydan A, Rosenbaum TY. War-Time Stress and Sexual Well-Being in Israel. International Journal of Sexual Health. 2024;36(1):1-14. doi: https://doi.org/10.1080/19317611.2024.2317169
27. Gul M, Bocu K, Serefoglu EC. Current and emerging treatment options for premature ejaculation. Nature reviews. Urology. 2022 Nov;19(11):659-80. doi: https://doi.org/10.1038/s41585-022-00639-5
28. Russo A, Capogrosso P, Ventimiglia E, La Croce G, Boeri L, Montorsi F, et al. Efficacy and safety of dapoxetine in treatment of premature ejaculation: an evidence-based review. Int J Clin Pract. 2016 Sep;70(9):723-33. doi: https://doi.org/10.1111/ijcp.12843
29. Gillman N, Gillman M. Premature Ejaculation: Aetiology and Treatment Strategies. Medical Sciences. 2019;7(11):102. doi: https://doi.org/10.3390/medsci7110102
30. Zhou Z, Yang Z, Cui Y, Zhang X, Wang Y, Zhang Y. The network meta-analysis of “on-demand” and “daily” use of paroxetine in treating men with premature ejaculation from randomized controlled trials. Andrologia. 2022;54: e14388. doi: https://doi.org/10.1111/and14388
31. Cortese F, Costantino MF, Luzi G. Can We Consider Erectile Dysfunction as an Early Markerof Cardiovascular Disease? JACC Adv. 2023;2(4):100384. doi: https://doi.org/10.1016/j.jacadv.2023.100384
32. Chéhensse C, Facchinetti P, Bahrami S, Andrey P, Soler JM, Chrétien F, et al. Human spinal ejaculation generator. Ann Neurol. 2017 Jan;81(1):35-45. doi: https://doi.org/10.1002/ana.24819
33. Chow J, Thompson AJ, Iqbal F, Zaidi W, Syed NI. The antidepressant sertraline reduces synaptic transmission efficacy and synaptogenesis between identified lymnaea neurons. Front Mar Sci. 2020;7:603789. doi: https://doi.org/10.3389/fmars.2020.603789
34. Yuan S, Deban CE. SSRI-Induced Hypersexuality. Am J Psychiatry Resid J. 2021 Mar;16(3):9-12. doi: https://doi.org/10.1176/appi.ajp-rj.2021.160305
35. Vorobets DZ, Fafula RV, Chaplyk VV, Vorobets MZ, Onufrovych OK, Besedina AS, et al. Erectile dysfunction and quality of life of men affected by hostilities in the Russian-Ukrainian war. Regulatory Mechanisms in Biosystems. 2024;15(1):62-6. doi: https://doi.org/10.15421/022409