
 UK
UK  EN
EN 

S. Belisha (Hoti)1
![]() I. Zekja2
I. Zekja2
![]() O. Petri3
O. Petri3
![]() B. Brati (Kika)4
B. Brati (Kika)4
![]() E. Fresku1
E. Fresku1
![]() E. Ali2
E. Ali2
![]() J. Kraja1
J. Kraja1
![]() Gj. Koja5
Gj. Koja5
![]() E. Abazaj *2
E. Abazaj *2
![]()
Key words: nursing staff, burnout professional, predisposing factor, syndrome, sociodemographic factors, work-related factors
Ключові слова: медсестринський персонал, професійне вигорання, фактор схильності, синдром, соціально-демографічні фактори, фактори, пов’язані з роботою
Abstract
This study aims to investigate the prevalence of occupational burnout among nursing professionals at Shkodra Regional Hospital and identify factors contributing to it. Specifically, the objectives include measuring the burnout rate within this population and analysing demographic and occupational factors that affect burnout levels. This cross-sectional, observational and analytical study used a semi-standardised questionnaire distributed to healthcare professionals over 7 months (September 2024 – March 2025) at the Shkodra Regional Hospital, Albania. The Excel file obtained from Microsoft software underwent statistical processing in SPSS version 26.0 software. The Maslach Burnout Inventory test was subjected to an evaluation of its reliability and consistency with the Cronbach alpha test. The alpha value was found to be 0.79. The level of significance adopted was p<0.05. The mean age among 131 nurses was 35.35±10.37, with a minimum to maximum age of 18-64 years old. Almost 38.2% of the participants belong to the 26-35 age group, which is considered to be a relatively young demographic one. Burnout prevalence turned to be relatively high – 68.9% for 95% CI (59.4-75.3), where 22.3% exhibited high levels of emotional exhaustion, 45.4% of cases high depersonalisation and low personal accomplishment domen in 92.3%. The phenomenon of depersonalization, in combination with two other areas, is worthy of consideration, with a p-value was found to be less than 0.05. It is noteworthy that the majority of these workers, 62.6%, are engaged in shift work with a frequency of 6-10 days per month. Burnout syndrome presented a correlation with sociodemographic factors (marital status, and monthly income) as well as some of the work-related factors (shift work system, weekly working hours, days on shift, work experience, etc). The findings of this study give us a relatively high prevalence of burnout syndrome among the participants (68.9%). We recommend rapid intervention with different policies or strategies that should improve the reduction of burnout among nursing staff. In order to facilitate recovery, it is essential to address burnout, recognise signs of excessive physical fatigue, seek support from colleagues and therapists, set boundaries, and prioritise self-care.
Реферат
Поширеність професійного вигорання: перехресний аналіз серед фахівців з догляду за хворими в лікарнях. Белішa (Готі) С., Зекя І., Петрі О., Браті (Кіка) Б., Фреску Е., Алі Е., Края Дж., Коя Дж., Абазай Е. Це дослідження має на меті дослідити поширеність професійного вигорання серед медсестер у Шкодерській регіональній лікарні та визначити фактори, що сприяють цьому. Зокрема, цілі включають вимірювання рівня вигорання серед цієї групи населення та аналіз демографічних та професійних факторів, що впливають на рівень вигорання. У цьому перехресному, обсерваційному та аналітичному дослідженні використовувалася напівстандартизована анкета, розповсюджена серед медичних працівників протягом 7 місяців (вересень 2024 р. – березень 2025 р.) у Шкодерській регіональній лікарні, Албанія. Файл Excel, отриманий з програмного забезпечення Microsoft, пройшов статистичну обробку в програмному забезпеченні SPSS версії 26.0. Тест Маслаха на вигорання був оцінений щодо його надійності та узгодженості з альфа-тестом Кронбаха. Значення альфа становило 0,79. Прийнятий рівень значущості становив p<0,05. Серед 131 медсестри середній вік становив 35,35±10,37 року, з мінімальним та максимальним віком 18-64 роки. Майже 38,2% учасників належать до вікової групи 26-35 років, яка вважається відносно молодою демографічною групою. Поширеність вигорання виявилася відносно високою і становила 68,9% для 95% ДІ (59,4-75,3), де 22,3% демонстрували високий рівень емоційного виснаження, 45,4% випадків – високий рівень деперсоналізації та низький рівень особистих досягнень у 92,3%. Феномен деперсоналізації в поєднанні з двома іншими областями заслуговує на увагу, при цьому значення p менше 0,05. Варто зазначити, що більшість цих працівників, 62,6%, працюють позмінно з частотою 6-10 днів на місяць. Синдром вигорання корелював із соціально-демографічними факторами (сімейний стан та щомісячний дохід), а також деякими факторами, пов'язаними з роботою (система позмінної роботи, тижневий робочий час, кількість днів у зміні, досвід роботи тощо). Результати цього дослідження свідчать про відносно високу поширеність синдрому вигорання серед учасників (68,9%). Ми рекомендуємо швидке втручання з використанням різних політик або стратегій, які повинні знизити вигорання серед медсестер. Для сприяння одужанню важливо боротися з вигоранням, розпізнавати ознаки надмірної фізичної втоми, звертатися за підтримкою до колег і терапевтів, встановлювати межі та надавати пріоритет турботі про себе.
Burnout has not been characterised as a medical diagnostic category; instead it has been recognised as a psychological syndrome. The term “burnout” was first coined in the 1970s in the USA by Freudenberger, 1974 [1] and Maslach, 1976 [2]. However, the most precise definition was subsequently provided by Maslach and Jackson, 1981 [3], who specified it as “a syndrome of emotional exhaustion, depersonalisation and reduced personal accomplishment that can occur among individuals who do “people-work” of some kind”.
Despite its psychological underpinnings, in the long term, it exerts a direct and detrimental effect on the individual's health [4, 5]. The World Health Organisation (WHO) defines “Burnout” as “an occupational phenomenon resulting from the failure to manage prolonged exposure to chronic stressors in the workplace effectively” [6].
This term has been utilised within the occupational medicine area. The manifestation of burnout syndrome is observed to vary in its presentation across diverse professional contexts. The consequences of professional burnout have been observed to encompass a wide spectrum of effects, including individual health concerns and organisational issues. As posited by Belisha et al., 2025, burnout has been identified as a pervasive problem among medical personnel, particularly those engaged in nursing and general practice [7]. The syndrome has been documented to manifest through three main symptoms: emotional exhaustion, depersonalisation, and a diminished sense of personal accomplishment.
These symptoms are predominantly experienced by the majority of nursing staff [8]. The predominant cause of burnout is identified as emotional exhaustion. The condition is characterised by a persistent state of fatigue, insomnia, and overwhelming stress [9]. As proposed by Petersen et al., 2023, nurses who experience emotional exhaustion frequently encounter emotional and burnout severity [10], which can impede their capacity to cope effectively with the demands of their professional duties [10,11]. In a further study by Lwiza & Lugazia, 2022, the prevalence of burnout among healthcare professionals in developed countries was estimated to range from 40% to 55% [12]. Moreover, a report by the World Economic Forum on the prevalence of burnout in different populations resulted in the following figures for specific countries [13]: The data indicates that 57% of the cases are in the UK, 50% in the US, 37% in Spain, and 30% in Germany and France, respectively [13,14].
The following essay will provide a comprehensive overview of the relevant literature on the subject. In the context of the national present, the prevalence of burnout among medical personnel, with a particular emphasis on nursing staff, remains under-researched. The extant literature on the subject is limited to a handful of recent publications [7,8,15]. This study aims to investigate the prevalence of occupational burnout among nursing professionals at Shkodra Regional Hospital and identify factors contributing to it. Specifically, the objectives include measuring the burnout rate within this population and analysing demographic and occupational factors that affect burnout levels.
MATERIALS AND METHODS OF RESEARCH
This cross-sectional, observational and analytical study was conducted over a 7-month period (September 2024 – March 2025) at the Shkodra Regional Hospital using a semi-standardized questionnaire distributed to healthcare professionals (nurses and midwifery staff). In this study, it was initially determined that only nursing staff would be included, with the exclusion of any medical or auxiliary staff. The inclusion criteria are as follows: the study is open to registered nursing staff working full-time in the hospital setting. Additionally, the study is open to any staff, irrespective of gender, aged between 23 and 65 years, and with a minimum of six months' experience in nursing practice. Staff members who are willing to participate in the study and provide consent will be eligible to take part. The exclusion criteria are as follows: the target demographic group for this study comprises nursing students, interns, and nursing staff with less than six months of experience in nursing practice. The sample calculation was conducted utilising Medicalcul software, which is an online resource that specialises in numerical computations within the medical field. The anticipated response rate was estimated to be in excess of 50% of the total nursing population.
The calculation demonstrated that a minimum of 162 participants were required to complete the online questionnaire, ensuring a confidence level of 95% and a true value within a margin of error of ±5% of the measured value. The questionnaire was uploaded to Microsoft Office software, after which the link was disseminated to all nurses via the WhatsApp website, Messenger, Facebook, and personal e-mails. At the commencement of each month for a period of approximately three months, a reminder was dispatched to the participants to complete the questionnaire. Registered nurses who completed the questionnaires also completed and signed the consent forms. In conclusion, the data from 130 nurses, who had completed all the questions as requested by the working group, were analysed.
In order to assess the determinants of excessive burnout severity, data were collected on a range of sociodemographic variables including, but not limited to, age, sex, residence, marital status, number of family members, educational level and family income. In addition, information was collected on the characteristics and work experiences of the nursing staff in order to provide a comprehensive overview of the subject matter. The second questionnaire is the standardized Maslach Burnout Inventory (MBI), which was developed and validated by Maslach & Jackson in 1981 [3]. This questionnaire is regarded by many researchers as the gold standard for measuring and assessing burnout in different professions [16, 17, 18, 19]. Its high reliability and validity are well-documented. The MBI is comprised of three distinct sections. The initial section concerns Emotional Exhaustion (EE), whereby individuals present with symptoms of fatigue in the workplace, chronic fatigue, sleep disturbances, and physical ailments. The second section is dedicated to Depersonalisation (DP), which can be defined as a form of "dehumanisation" that manifests in interpersonal relationships. The third section of the questionnaire is entitled Personal Accomplishment (PA). In this section, individuals experience a diminution in PA, frequently receiving a negative appraisal and perceiving an inability to progress a situation. A high score in the first two sections and a low score in the last section may be indicative of burnout. It is imperative to note that all questions in this questionnaire are formulated as statements pertaining to personal sentiments or dispositions.
The frequency scale is labelled on each point, starting from 1 to 7, with 1=Never; 2=Few times a year; 3=Once a month; 4=Few times a month; 5=Once a week; 6=Few times a week; 7=Everyday. Following the adaptation of the questionnaire into Albanian, the translated version was evaluated by three specialists in the field. The evaluation was then conducted in a pilot study phase. Following the pilot phase and the implementation of minor linguistic modifications, the MBI test was subjected to an evaluation of its reliability and consistency with the Cronbach alpha test. The alpha value was found to be 0.79.
The initial step in commencing the work for this study was to apply to the ethics committee at the University of Medicine, Tirana, for approval. Firstly, all documentation related to the purpose of the study, the methodology to be employed, the expected results and the involvement of health workers was prepared. Subsequently, the documentation was submitted to the University of Medicine’s Ethics Committee in Tirana for the purpose of obtaining approval and authorisation for the study. Following the received ethical approval from the relevant committee, the investigators proceeded to present themselves to the hospital directorate at which the study was to be conducted. The individuals responsible for authorising and facilitating the execution of this study by the medical personnel have taken measures to ensure that the highest standards of research integrity have been adhered to. The working group convened a preliminary meeting with the employees, during which the purpose and objectives of the study were communicated to each participant. It was emphasised that participation in the study was voluntary and that employees were at liberty to withdraw from the study at any time. It was explained to each participant that no incentives or gifts would be offered. Each participant was assured of the maintenance and storage of the data, with confidentiality guaranteed for any data provided by them. The survey was completed within a time frame of over 30 minutes.
The Excel file obtained from Microsoft software underwent statistical processing in IBM Statistics software SPSS, version 26.0 Issue, DT449052. The data were presented as frequency and percentage, as well as mean and standard deviation (SD). The statistical analysis was conducted using a combination of student t-test, linear correlation, and linear regression analysis. In the context of categorical data, the statistical analysis employed was the chi-squared test. The level of significance adopted was p<0.05.
RESULTS AND DISCUSSION
In the context of this cross-sectional and descriptive study, it is important to reiterate the exclusionary criteria previously outlined in the methodology section. Specifically, the study focused exclusively on nursing and midwifery staff, with the former constituting 83.2% of the sample and the latter making up 16.8%. As illustrated in Table 1, the descriptive socio-demographic data of 131 medical personnel participants is presented, with a mean age of 35.35±10.37, a minimum age of 18 years, and a maximum of 64 years. The data indicates that almost 38.2% of the participants belong to the 26-35 age group, which is considered to be a relatively young demographic. The majority of the subjects are female, accounting for 71.8% of the total, and approximately 74.8% of the participants reside in urban areas. It is important to note that 28.2% of the participants in this study reside with family members, including spouses, children, and parents.
Furthermore, 27.5% of the participants live solely with parents, and it is noteworthy that the majority of these families consist of four to six members (58.2%). With respect to familial income, the majority of respondents (48.9%) reported a family income ranging from 60,001 to 100,000 lek (Table 1).
The second section of the questionnaire, which was drafted by the working group, concerns itself with the issue of employment data and the working hours that respondents perform on a daily basis at the Shkodra Regional Hospital. As anticipated, the vast majority of the participants, approximately 97.7%, are engaged in full-time employment at this institution, with a mere 2.3% engaged in part-time or temporary contractual arrangements.
With regard to the work experience of the medical staff (nurses and midwives), it is evident that a significant proportion of the sample, constituting 33.6% of the total, have length of service from one and five years of experience. However, it is noteworthy that the majority of these workers, 62.6%, are engaged in shift work, while only 37.4% adhere to a standard 8-hour workday. In this study, approximately 50% of the participants (49.6%) reported working on the second shift, with a frequency of 6-10 days per month. Meanwhile, 47.3% of the participants indicated that they worked on the third shift, with a frequency of 6-10 times per month.
Furthermore, it was observed that approximately one-third of the participants (29.8%) had been working in shifts for 1-5 years. A mere 9.2% of nurses and midwives have been working in shifts for less than one year, while 6.9% have been working in shifts for more than 20 years (Table 2).
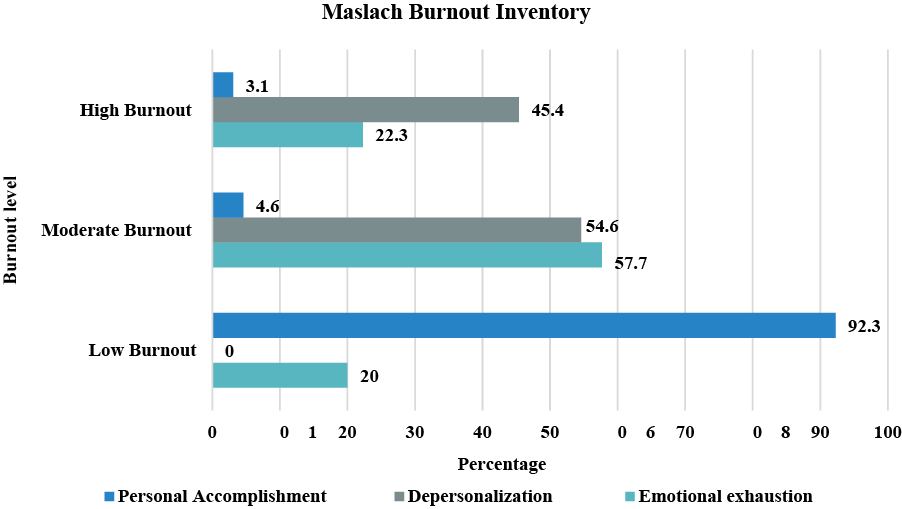
The following figure presents the levels of burnout experienced by nursing staff for each of the MBI test areas. In the context of the "Emotional Exhaustion" area, 22.3% of the nursing staff exhibited high levels of burnout, while 57.7% demonstrated moderate symptoms. Notably, only 20% of the participants exhibited low levels of burnout. In the case of the “Depersonalisation” area, 45.4% of cases resulted in high levels of burnout, while 54.6% resulted in moderate levels. There were no cases of low burnout. With regard to the “Personal Accomplishment” area, 3.1% of subjects have been identified as experiencing high levels of burnout, 4.6% are exhibiting moderate symptoms, and 92.3% demonstrate low levels of burnout (Fig.).
Variables Categories Frequency Percentage Age group (years) ≤25 years old 25 19.1 26-35 years old 50 38.2 36-45 years old 31 23.7 46-55 years old 18 13.7 56-65 years old 7 5.3 Gender Male 37 28.2 Female 94 71.8 Residence Rural area 33 35.2 Urban area 98 74.8 Marital status Relationship 3 2.3 Single 37 28.2 Divorced 1 0.8 Married 89 68 I/e widow 1 0.8 Education level Higher education 129 98.4 Secondary education 2 1.6 How many members are in your family 1-3 members 36 27.6 4-6 members 76 58.2 ≥7 members 19 14.6 Monthly family income level less than 40,000 lek 2 1.6 40,001-60,000 lek 22 16.8 60,001-100,000 lek 64 48.9 more than 100,001 lek 43 32.8
(exact number)
The following table illustrates the correlation statistics of the scores collected for the three MBI areas. As demonstrated in Table 3, a positive correlation between emotional exhaustion and depersonalisation is evident. Furthermore, DP has been found to correlate with both EM and PA, nonetheless, a negative correlation is evident in the latter case. The phenomenon of depersonalization, in conjunction with two other areas, is worthy of consideration. In all cases, the p-value was found to be less than 0.05 (Table 3).
Correlations Emotional Exhaustion Depersonalization Personal Accomplishment Emotional Exhaustion Pearson Correlation 1 0.528** -0.046 Sig. (2-tailed) 0.000 0.601 Depersonalization Pearson Correlation 0.528** 1 -0.395** Sig. (2-tailed) 0.000 0.000 Personal Achievements Pearson Correlation -0.046 -0.395** 1 Sig. (2-tailed) 0.601 0.000 Notes: * – correlation is significant at the 0.05 level (2-tailed); ** – correlation is significant at the 0.01 level (2-tailed).
In the subsequent table, we have presented the correlations between risk factors and the extent of burnout, according to each area. As is apparent from the data, a significant relationship (positive/negative) is observed between one, two or three domens and several factors, including marital status, family monthly income, employment status, profession, work system, hours of work based on the work system, and the number of times the third shift is worked. The issue of staff shortages, necessitating the replacement of other personnel, is one that is frequently encountered. The question of being overloaded at work is also one that is pertinent. The purpose of this study is to ascertain the level of job satisfaction experienced by respondents. The present study seeks to ascertain whether respondents are satisfied with the conditions of their working environment. What is the nature of your relationship with your colleagues? The final question pertains to the question of whether the individual in question has the support of their superiors in their professional endeavours. In all cases, the p-value was found to be less than 0.05 (Table 4).
Factors correlations Emotional Exhaustion Depersonalization Personal Accomplishment Gender Pearson Correlation 0.006 0.108 -0.153 Sig. (2-tailed) 0.944 0.223 0.083 Residence Pearson Correlation -0.034 0.011 0.023 Sig. (2-tailed) 0.703 0.897 0.795 Marital Status Pearson Correlation 0.363 0.486 -0.394 Sig. (2-tailed) 0.003 0.000 0.008 Educatio level Pearson Correlation -0.037 -0.081 0.065 Sig. (2-tailed) 0.674 0.362 0.461 How many members are in your family Pearson Correlation -0.022 0.084 0.075 Sig. (2-tailed) 0.807 0.341 0.394 Family monthly income level Pearson Correlation -0.357 0.305 0.346 Sig. (2-tailed) 0.006 0.025 0.006 Employes status Pearson Correlation -0.068 0.028 -0.185* Sig. (2-tailed) 0.444 0.754 0.035 Profession Pearson Correlation -0.196* -0.171 0.112 Sig. (2-tailed) 0.025 0.052 0.207 Work system Pearson Correlation -0.297 0.274 0.326 Sig. (2-tailed) 0.012 0.045 0.009 The hours you work are based on the work system Pearson Correlation 0.389** 0.302** -0.159 Sig. (2-tailed) 0.005 0.004 0.07 Working time days/hours Pearson Correlation 0.498** 0.245** -0.130 Sig. (2-tailed) 0.000 0.008 0.125 How many times in month are you on second shift Pearson Correlation 0.139 0.089 0.067 Sig. (2-tailed) 0.234 0.234 0.395 How many times are you on the third shift Pearson Correlation 0.321 0.373 0.285 Sig. (2-tailed) 0.008 0.003 0.045 How many years have you been working shifts Pearson Correlation -0.421** -0.328** .345** Sig. (2-tailed) 0.000 0.000 0.001 Do you often face staff shortages where you have to replace other people? Pearson Correlation 0.321** 0.249** -0.002 Sig. (2-tailed) 0.000 0.004 0.983 Are you overloaded at work? Pearson Correlation 0.434** 0.230** -0.104 Sig. (2-tailed) 0.000 0.008 0.241 Have you been absent from work for health reasons Pearson Correlation 0.113 0.108 0.032 Sig. (2-tailed) 0.201 0.223 0.714 How satisfied are you with your job Pearson Correlation -0.414** -0.399** .286** Sig. (2-tailed) 0.000 0.000 .001 Are you satisfied with the conditions of the environment where you work Pearson Correlation -0.281** -0.230** .094 Sig. (2-tailed) 0.001 0.008 0.288 What is your relationship with colleagues Pearson Correlation -0.341** -0.289** 0.364 Sig. (2-tailed) 0.000 0.001 0.003 Do you have the support of your superiors in your work? Pearson Correlation -0.344** -0.389** 0.269 Sig. (2-tailed) 0.000 0.000 0.045 Notes: * – correlation is significant at the 0.05 level (2-tailed); ** – correlation is significant at the 0.01 level (2-tailed).
Burnout, a syndrome that has the potential to affect healthcare systems on a global scale, has been referred to as the "disease of the 21st century" [7]. The issue of excessive burnout severity in our country has not been the focus of significant research interest, resulting in a paucity of analysis and examination of the predisposing factors that contribute to it. The present study examines the prevalence of the aforementioned syndrome and its correlation with socio-demographic and professional variables that contribute to the condition among healthcare personnel (nursing). The prevalence of burnout among 131 nurses was found to be relatively high at 68.9%, with a 95% confidence interval of [59.4 to 75.3]. The mean value of the EE area was found to be 24.59 for 95% CI [19 to 30], while the participants with the highest EE resulted in 22.3%. The mean value of DP resulted in 13.04 for 95% CI [8-16], where 45.4% of the participants appear to have high DP. The mean value for the PA area was found to be 53%, with a 95% confidence interval of [48.5 to 56]. This indicates a prevalence of low PA, with 92.3% of the participants demonstrating this level of physical activity. This value is relatively high, as demonstrated by a study conducted by Heinen et al., which assessed the prevalence of burnout in 10 European countries. This prevalence was on an average of 28% of nursing staff, where the lowest prevalence was observed in employees in the Netherlands with 10% and the highest in employees in England with 42% [20]. Conversely, the prevalence observed in this study was lower than that reported by Mathkour et al., who found a prevalence rate of burnout among healthcare workers in 73.3% of participants [21]. A substantial body of research has identified various sociodemographic factors [e.g., gender, marital status] and work-related factors [e.g., weekly work hours, monthly night shifts, years of experience, sleep quality, depressive symptoms, anxiety symptoms] as significant contributors to the development of high burnout [22, 23, 24]. In relation to factors such as gender, research indicates that women are more likely to experience physical fatigue syndrome than men [25]. The present study found no significant relationship, which is consistent with the findings of another study [12]. The impact of marital relationships and family stability on individual lives has been demonstrated to be a positive one.
Conversely, an unstable relationship has been shown to engender stress, which can in turn compromise work performance and quality of life [26, 27]. This, in turn, has the potential to increase the risk of burnout syndrome. The findings of this study revealed no significant relationship between burnout and marital status, a finding that aligns with the results of a previous study [26, 27]. A number of studies have indicated that the combination of factors, including extended working hours, shift work systems, protracted work hours, work experience, relationships with colleagues and superiors, frequently contributes to elevated levels of stress among employees, who often report a high degree of burnout [24-28]. In the majority of cases, these employees are potentially vulnerable groups susceptible to excessive fatigue.
The findings of the present study are consistent with those of previous studies, for some of the variables such as marital status, family monthly income, profession, work systems, weekly hours at work, working time days/hours, etc. For each of these variables, a strong correlation was identified between one, two or three areas of the MBI questionnaire, with a p value less than 0.05%. It is imperative to acknowledge the limitations of this study when interpreting the findings. Firstly, the number of nursing staff included was minimal. Secondly, the study focuses exclusively on nursing staff, excluding all other medical personnel. This methodological decision is pivotal in enabling a meaningful comparison between the two groups. Thirdly, the decision was taken to utilise the method of data collection through self-reported questionnaires. However, the reliability of this method of completion is questionable, given the observed discrepancy between cases that refer to depersonalisation and those that demonstrate low personal achievement in their work. This discrepancy may introduce a degree of bias into the responses. Notwithstanding the aforementioned limitations, the study successfully achieved its objectives and constitutes a valuable resource as it is the inaugural study to investigate the prevalence of burnout syndrome and its associated factors among healthcare workers in Shkoder.
CONCLUSION
1. This study has determined a relatively high prevalence rate (68.9%) of burnout syndrome within the surveyed population. A significant proportion of the nursing staff exhibited elevated levels of burnout in the Depersonalisation area, with 45.4% demonstrating high Emotional Exhaustion and 24.59% exhibiting low Personal Accomplishment.
2. The present study identified several factors that were found to be significantly associated with burnout syndrome. These factors included sociodemographic factors, such as marital status and monthly income, as well as work-related factors, including shift work system, weekly working hours, days on shift, and work experience.
3. In order to facilitate recovery, it is essential to address burnout, recognise signs of excessive physical fatigue, seek support from colleagues and therapists, set boundaries, and prioritise self-care.
4. In view of the high prevalence of burnout, it is recommended that prompt intervention be made with various policies or strategies that should lead to a reduction in the incidence of burnout among nursing staff.
5. Achieving an equilibrium between opportunities and work performance is a crucial factor in effective stress management, which will reduce burnout and enhancement of quality of life among healthcare workers. In addition to this, a superior standard of patient care is provided.
Contributors:
Belisha (Hoti) S. – conceptualization, methodology, investigation, project administration, writing – review & editing;
Zekja I. – project administration, supervision, methodology, writing – review & editing;
Petri O. – methodology, investigation, data curation, writing – original draft, formal analysis;
Brati (Kika) B. – methodology, formal analysis, investigation, data curation, writing – original draft;
Fresku E. – data curation, formal analysis, supervision, writing – original draft;
Ali E. – supervision, methodology, investigation, writing – review & editing;
Kraja J. – methodology, investigation, formal analysis, writing – review & editing;
Koja Gj. – investigation, formal analysis, writing – original draft;
Abazaj E. – conceptualization, methodology, investigation, project administration, data curation, formal analysis, supervision, writing – original draft; writing – review & editing.
Acknowledgements
It is imperative to express our profound gratitude to all those members of staff whose invaluable contributions were instrumental in the design, implementation and completion of this study. Secondly, gratitude is extended to all nursing staff of Rajonal Hospital of Shkodra, who participated in this study, responding promptly to the invitation and completing the form in an expeditious manner.
Funding. This research received no external funding.
Conflict of interests. The authors declare no conflict of interest.
REFERENCES
1. Freudenberger HJ. Staff Burn-Out. Journal of Social Issues. 1974;30(1):159-65. doi: https://doi.org/10.1111/j.1540-4560.1974.tb00706.x
2. Maslach C. Burned out. Human Behavior. [Internet]. 1976 [cited 2025 Aug 23];59:16-22. Available from: https://www.researchgate.net/publication/263847499_Burned-Out
3. Maslach C, Jackson SE. The measurement of experienced burnout. Journal of Occupational Psychology. 1981;2(2):99-113. doi: https://doi.org/10.1002/job.4030020205
4. Barragán Martín AB, Molero Jurado MDM, Pérez-Fuentes MDC, Simón Márquez MDM, Sisto M, Gázquez Linares JJ. Published research on burnout in nursing in Spain in the last decade: bibliometric analysis. Healthcare (Basel). 2020 Nov 12;8(4):478. doi: https://doi.org/10.3390/healthcare8040478
5. Nagarajan R, Ramachandran P, Dilipkumar R, Kaur P. Global estimate of burnout among the public health workforce: A systematic review and meta-analysis. Human Resources for Health. 2024;22:30. doi: https://doi.org/10.1186/s12960-024-00917-w
6. World Health Organization. Burn-out an "occupational phenomenon": International Classification of Diseases [Internet]. 2022 [cited 2025 Aug 23]. Available from: https://www.who.int/news/item/28-05-2019-burn-outan-occupational-phenomenon-international-classification-of-diseases
7. Belisha S, Zekja I, Abazaj E, Dibra V. Prevalence and associated risk factors for occupational burnout among healthcare personnel: a systematic review. Albanian Journal of Trauma and Emergency Surgery. 2025;9(2):1852-62. doi: https://doi.org/10.32391/ajtes.v9i2.448
8. Ramasaco L, Abazaj E, Brati B. Mental Health Burden among Healthcare Workers during the COVID-19 Time in Albania. ASEAN Journal of Psychiatry. 2023;24(1);1-13. doi: https://doi.org/10.54615/2231-7805.47289
9. Butler S. Understanding burnout in nurses: Identification and coping strategies. British Journal of Nursing. 2025;34(4):220-4. doi: https://doi.org/10.12968/bjon.2024.0244
10. Petersen J, Wendsche J, Melzer M. Nurses’ emotional exhaustion: Prevalence, psychosocial risk factors and association to sick leave depending on care setting: a quantitative secondary analysis. J Adv Nurs. 2023;79(1):182-93. doi: https://doi.org/10.1111/jan.15471
11. Kelly L. Burnout, compassion fatigue, and secondary trauma in nurses: recognising the occupational phenomenon and personal consequences of caregiving. Crit Care Nurs Q. 2020;43(1):73-80. doi: https://doi.org/10.1097/CNQ.0000000000000293
12. Lwiza AF, Lugazia ER. Burnout and associated factors among healthcare workers in acute care settings at a tertiary teaching hospital in Tanzania: An analytical cross-sectional study. Health science reports. 2023;6:e1256. doi: https://doi.org/10.1002/hsr2.1256
13. World Economic Forum. Wellbeing and Mental Health. What causes us to burnout at work? [Internet]. 2019 Oct 10 [cited 2025 Aug 23]. Available from: https://www.weforum.org/stories/2019/10/burnout-mental-health-pandemic/
14. Woo T, Ho R, Tang A, Tam W. Global prevalence of burnout symptoms among nurses: A systematic review and meta-analysis. J Psychiatr Res. 2020;123:9-20. doi: https://doi.org/10.1016/j.jpsychires.2019.12.015
15. Merkuri L, Paja E, Hoxhallari K. Burnout among nursing staff: an overview of causes, consequences, and management strategies. MEDICUS. 2025;9(1):38-45. doi: https://doi.org/10.58944/ycqo2677
16. Abdo SAM, El-Sallamy RM, El-Sherbiny AAM, Kabbash IA. Burnout among physicians and nursing staff working in the emergency hospital of Tanta University, Egypt. Eastern Mediterranean Health Journal La Revue de Santé de la Méditerranée orientale. 2015;21(12):906-15. doi: https://doi.org/10.26719/2015.21.12.906
17. Suner-Soler R, Grau-Martína A, Flichtentrei D, Prats M, Braga F, Font-Mayolas S, et al. The consequences of burnout syndrome among healthcare professionals in Spain and Spanish speaking Latin American countries. Burnout Res. 2014;1:82-89. doi: https://doi.org/10.1016/j.burn.2014.07.004
18. Chou LP, Li CY, Hu SC. Job stress and burnout in hospital employees: comparisons of different medical professions in a Regional hospital in Taiwan. BMJ Open. 2014;4:e004185.
doi: https://doi.org/10.1136/bmjopen-2013-004185
19. Schuttle N, Toppinen S, Kalimo R, Schaufeli W. The factorial validity of the Maslach Burnout Inventory across oc cupational groups and nations. J Occup Organ Psychol. 2000;73:53-66. doi: https://doi.org/10.1348/096317900166877
20. Heinen MM, van Achterberg T, Schwendimann R, Zander B, Matthews A, Kózka M, et al. Nurses' intention to leave their profession: a cross sectional observational study in 10 European countries. Int J Nurs Stud. 2013;50:174-84. doi: https://10.1016/j.ijnurstu.2012.09.019
21. Mathkour A, Alzahrani AH, Narapureddy BR, Alqahtani FM, Alshehri AM, Althagafi MA, et al. Prevalence and risk factors of burnout among employees at COVID-19 vaccination centers: A cross sectional study. PloS One. 2025;20(5):e0322803. doi: https://doi.org/10.1371/journal.pone.0322803
22. Zhang X, Wang J, Hao Y, Wu K, Jiao M, Liang L, et al. Prevalence and Factors associated with burnout of frontline healthcare workers in fighting against the COVID-19 Pandemic: Evidence from China. Front Psychol. 2021;12:680614. doi: https://doi.org/10.3389/fpsyg.2021.680614
23. Mohamed NA, Mohamed YA, Haji Mohamud RY, Gabow AA. Evaluation of the prevalence and risk factors of burnout syndrome among healthcare workers: A cross-sectional study. World J Psychiatry. 2025;15(2):98496. doi: https://doi.org/10.5498/wjp.v15.i2.98496
24. Lee YL, Dai JW, Li XW, et al. Prevalence and the associated factors of burnout among the critical healthcare professionals during the post-pandemic era: a multi-institutional survey in Taiwan with a systematic review of the Asian literatures. BMC Public Health. 2024;24:3480. doi: https://doi.org/10.1186/s12889-024-21084-6
25. Anbesaw T, Zenebe Y, Abebe M, Tegafaw T. Burnout Syndrome and Associated Factors Among Health Care Professionals Working in Dessie Comprehensive Specialized Hospital, Dessie, Ethiopia. Sage Open. 2023;13(4):1-9. doi: https://doi.org/10.1177/21582440231215147
26. Dechasa DB, Worku T, Baraki N, Merga BT, Asfaw H. Burnout and associated factors among nurses working in public hospitals of Harari region and Dire Dawa administration, eastern Ethiopia. A cross sectional study. PloS One. 2021;16:e0258224. doi: https://doi.org/10.1371/journal.pone.0258224
27. Chirico F, Afolabi AA, Ilesanmi OS, Nucera G, Ferrari Ge, Sacco A, et al. Prevalence, risk factors and prevention of burnout syndrome among healthcare workers: An umbrella review of systematic reviews and meta-analyses. Journal of Health and Social Sciences. 2021;6(4):465-91. doi: https://doi.org/10.19204/2021/prvl3
28. Merces MCD, Coelho JMF, Lua I, Silva DSE, Gomes AMT, Erdmann AL, et al. Prevalence and factors associated with burnout syndrome among primary health care nursing professionals: a cross sectional study. Int J Environ Res Public Health. 2020;17(2):474. doi: https://doi.org/10.3390/ijerph17020474